

Use of Modeling and Simulations to Determine Raltegravir Dosing in Neonates: A Model for Safely and Efficiently Determining Appropriate Neonatal Dosing Regimens: IMPAACT P1110
- PMID: 31658182
- PMCID: PMC6820708
- DOI: 10.1097/QAI.0000000000002149
Use of Modeling and Simulations to Determine Raltegravir Dosing in Neonates: A Model for Safely and Efficiently Determining Appropriate Neonatal Dosing Regimens: IMPAACT P1110
Abstract
Background: Population modeling and simulations can be used to facilitate the conduct of phase I studies to develop safe and effective dosing regimens in neonates.
Setting: P1110 is an international, multicenter trial to determine safe and effective raltegravir doses in neonates at risk for HIV infection.
Methods: P1110 used a 2-cohort adaptive design incorporating population pharmacokinetic modeling and simulations. An initial cohort of neonates received 2 single oral doses of raltegravir with standard-of-care therapy for prevention of perinatal transmission-one within 48 hours of birth and a second at 7-10 days of life. Raltegravir concentration data after administration of these doses were combined with data from a previous study of infants aged 4 weeks to 2 years. The combined database was used for population pharmacokinetic modeling and simulations to select a daily dosing regimen for investigation in a second cohort of neonates.
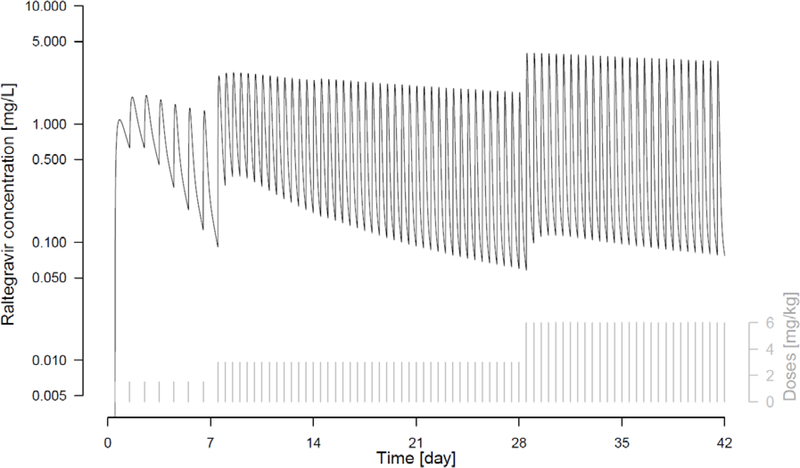
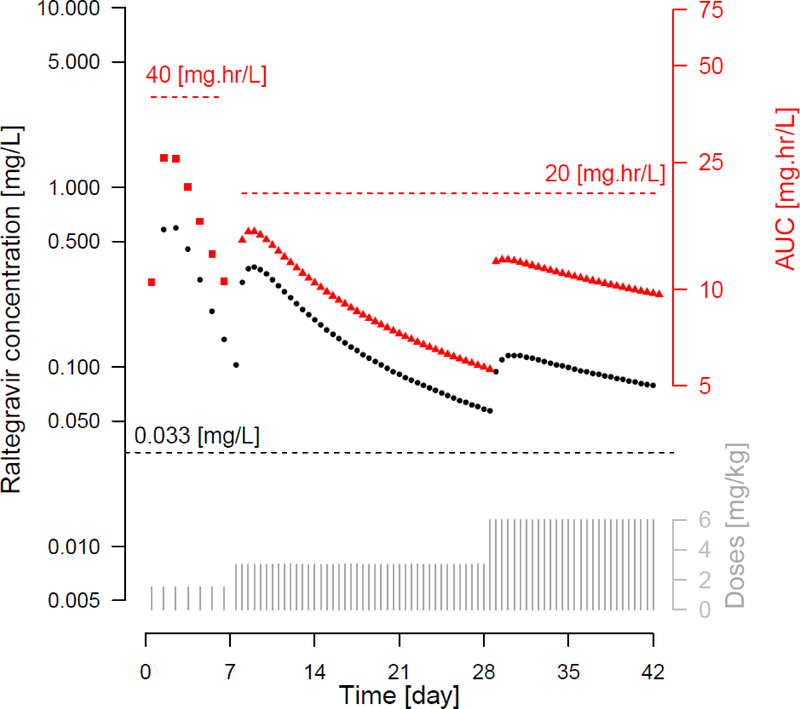
Results: Raltegravir concentration data from 6 neonates were combined with data from infants aged 4 weeks to 2 years receiving raltegravir twice daily. The combined data set allowed for successful development of a population pharmacokinetic model with reasonable precision of parameter estimates. Monte Carlo simulations were run to evaluate potential daily dosing regimens from birth to 6 weeks of age, allowing for selection of a regimen to be evaluated in a subsequent cohort of neonates receiving chronic raltegravir dosing.
Conclusions: An adaptive design incorporating population pharmacokinetic modeling and simulations was used to select a developmentally appropriate neonatal raltegravir dosing regimen in the first 6 weeks of life.
Figures
References
-
- Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission. Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/PerinatalGL.pdf. Accessed (October 8, 2018).
-
- Panel on Antiretroviral Therapy and Medical Management of Children Living with HIV. Guidelines for the Use of Antiretroviral Agents in Pediatric HIV Infection. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/pediatricguidelines.pdf. Accessed (November 18, 2018).
-
- Krekels EH, Danhof M, Tibboel D, Knibbe CA. Ontogeny of hepatic glucuronidation; methods and results. Curr Drug Metab. July 2012;13(6):728–743. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
