

Association Between Diagnoses of Chronic Noncancer Pain, Substance Use Disorder, and HIV-Related Outcomes in People Living With HIV
- PMID: 31658202
- PMCID: PMC6822377
- DOI: 10.1097/QAI.0000000000002179
Association Between Diagnoses of Chronic Noncancer Pain, Substance Use Disorder, and HIV-Related Outcomes in People Living With HIV
Abstract
Background: Chronic pain is common in people living with HIV (PLWH). Few studies have evaluated the association between the diagnoses of chronic pain, substance use disorder (SUD), and HIV-related outcomes in clinical settings over a 10-year period.
Methods: Using electronic medical records, the study described psychiatric diagnoses, pain medication, and HIV-related variables in PLWH and examined the factors associated with pain diagnosis and HIV-related outcomes.
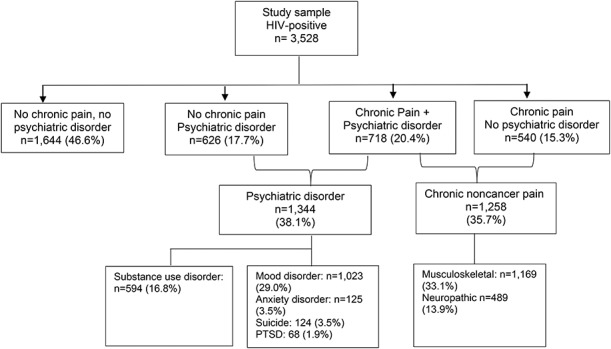
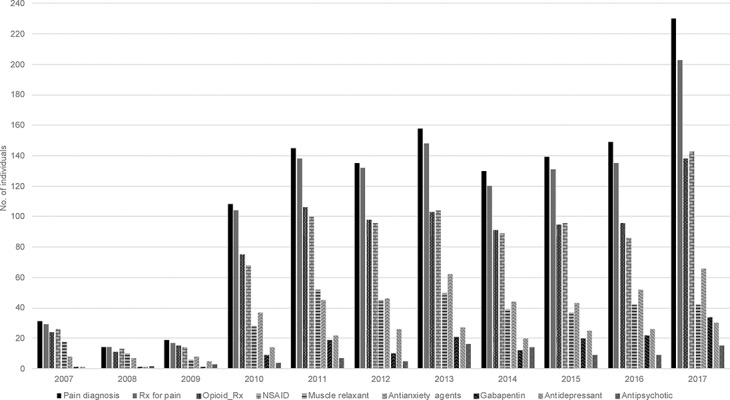
Results: Among 3528 PLWH, more than one-third exhibited a chronic pain diagnosis and more than one-third a psychiatric disorder. Chronic pain diagnosis has been associated with SUD and mood and anxiety disorders and occurred before SUD or psychiatric disorders about half of the time. Opioids have been commonly prescribed for pain management, more often than nonopioid analgesic, without any change in prescription pattern over the 10-year period. A dual diagnosis of pain and SUD has been associated with more psychiatric disorders and had a negative impact on the pain management by requesting more health care utilization and higher frequency of both opioid and nonopioid medication prescriptions. Chronic pain and SUD had a negative impact on ART adherence. SUD but not chronic pain has been associated with an unsuppressed HIV viral load.
Conclusions: In the current intertwining opioid prescription and opioid epidemic, opioids are still commonly prescribed in PLWH in HIV care. A diagnosis of chronic pain and/or SUD worsened the HIV-related outcomes, emphasizing the potential risk of the HIV epidemic. These findings called for a better coordinated care program in HIV clinics.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Krashin DL, Merrill JO, Trescot AM. Opioids in the management of HIV-related pain. Pain Physician. 2012;15(3 suppl):ES157–168. - PubMed
-
- Jiao JM, So E, Jebakumar J, et al. Chronic pain disorders in HIV primary care: clinical characteristics and association with healthcare utilization. Pain. 2016;157:931–937. - PubMed
