

A management algorithm for patients with intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC)
- PMID: 31659383
- PMCID: PMC6863785
- DOI: 10.1007/s00134-019-05805-9
A management algorithm for patients with intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC)
Abstract
Background: Management algorithms for adult severe traumatic brain injury (sTBI) were omitted in later editions of the Brain Trauma Foundation's sTBI Management Guidelines, as they were not evidence-based.
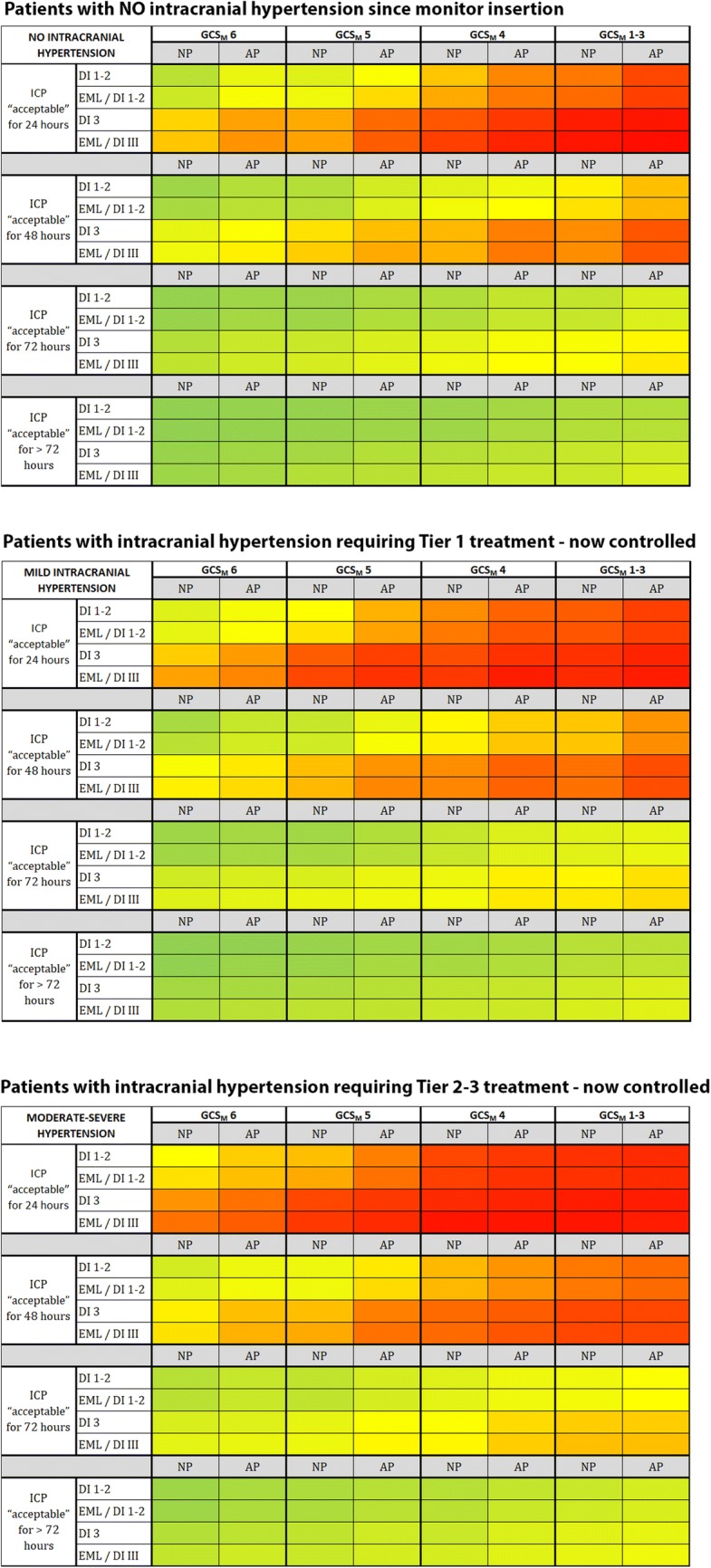
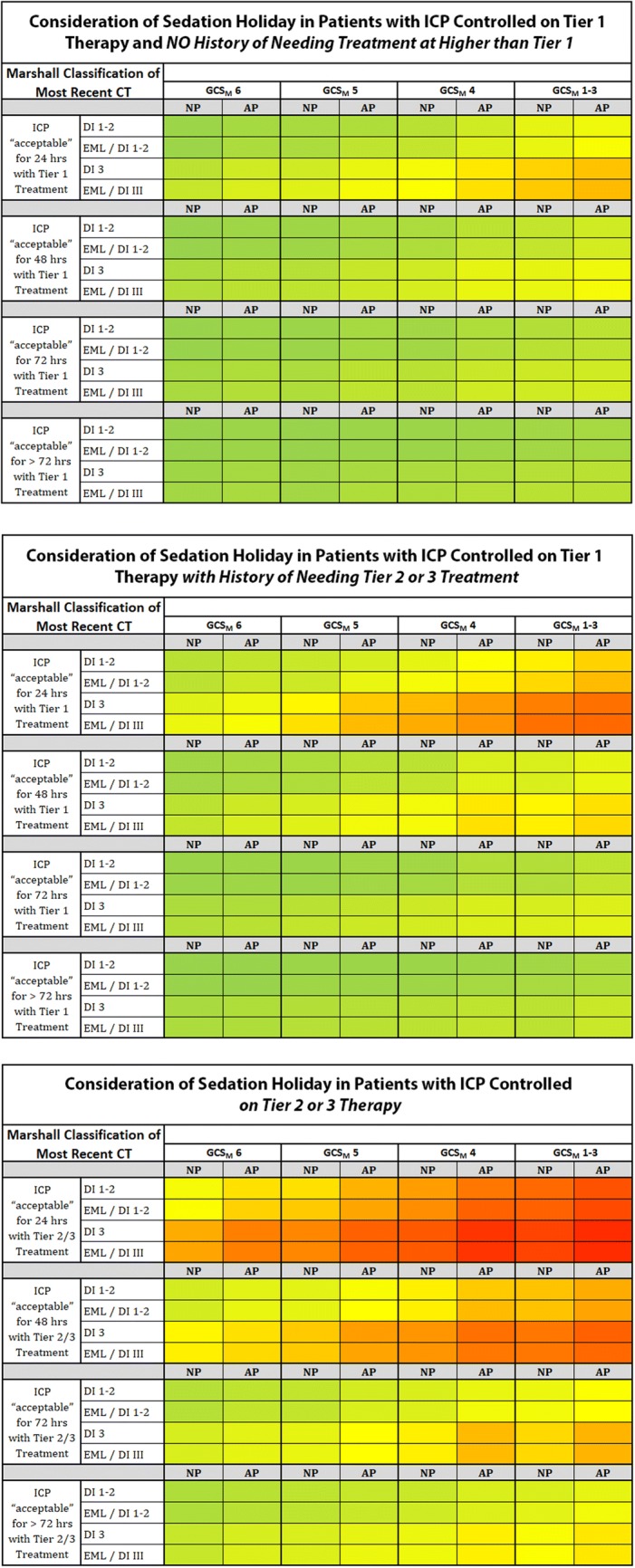
Methods: We used a Delphi-method-based consensus approach to address management of sTBI patients undergoing intracranial pressure (ICP) monitoring. Forty-two experienced, clinically active sTBI specialists from six continents comprised the panel. Eight surveys iterated queries and comments. An in-person meeting included whole- and small-group discussions and blinded voting. Consensus required 80% agreement. We developed heatmaps based on a traffic-light model where panelists' decision tendencies were the focus of recommendations.
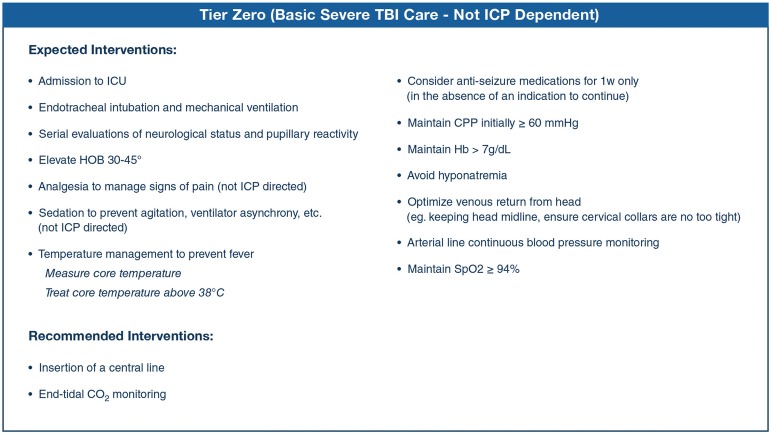
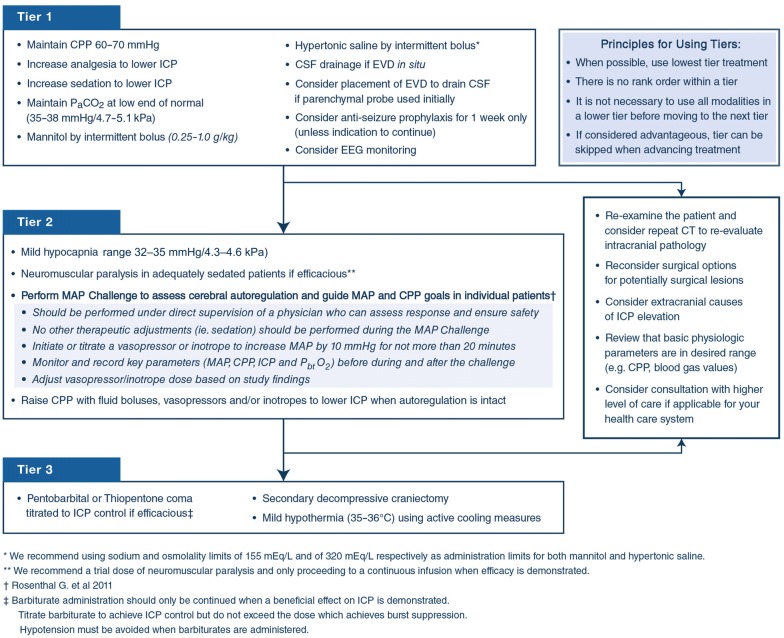
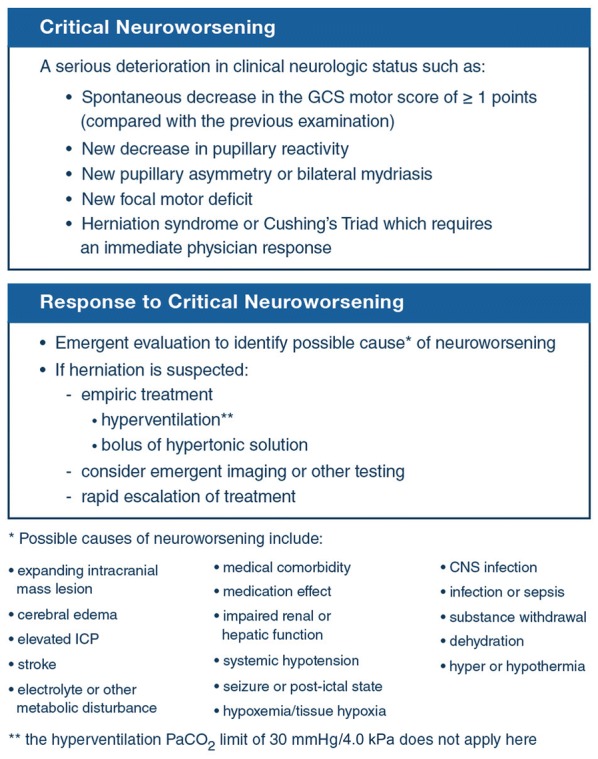
Results: We provide comprehensive algorithms for ICP-monitor-based adult sTBI management. Consensus established 18 interventions as fundamental and ten treatments not to be used. We provide a three-tier algorithm for treating elevated ICP. Treatments within a tier are considered empirically equivalent. Higher tiers involve higher risk therapies. Tiers 1, 2, and 3 include 10, 4, and 3 interventions, respectively. We include inter-tier considerations, and recommendations for critical neuroworsening to assist the recognition and treatment of declining patients. Novel elements include guidance for autoregulation-based ICP treatment based on MAP Challenge results, and two heatmaps to guide (1) ICP-monitor removal and (2) consideration of sedation holidays for neurological examination.
Conclusions: Our modern and comprehensive sTBI-management protocol is designed to assist clinicians managing sTBI patients monitored with ICP-monitors alone. Consensus-based (class III evidence), it provides management recommendations based on combined expert opinion. It reflects neither a standard-of-care nor a substitute for thoughtful individualized management.
Keywords: Algorithm; Brain injury; Consensus; Head trauma; Intracranial pressure; Protocol; SIBICC; Seattle; Tiers.
Conflict of interest statement
No conflicts of interest relevant to this project were identified amongst the authorship group.
Figures
Comment in
-
An algorithm for patients with intracranial pressure monitoring: filling the gap between evidence and practice.Intensive Care Med. 2019 Dec;45(12):1819-1821. doi: 10.1007/s00134-019-05818-4. Epub 2019 Oct 15. Intensive Care Med. 2019. PMID: 31616963 No abstract available.
References
-
- Brain Trauma F, American Association of Neurological S, Congress of Neurological S, Joint Section on N, Critical Care AC. Carney NA, Ghajar J. Guidelines for the management of severe traumatic brain injury. Introduction. J Neurotrauma. 2007;24(Suppl 1):S1–S2. - PubMed
