

General treatment principles for fracture-related infection: recommendations from an international expert group
- PMID: 31659475
- PMCID: PMC7351827
- DOI: 10.1007/s00402-019-03287-4
General treatment principles for fracture-related infection: recommendations from an international expert group
Abstract
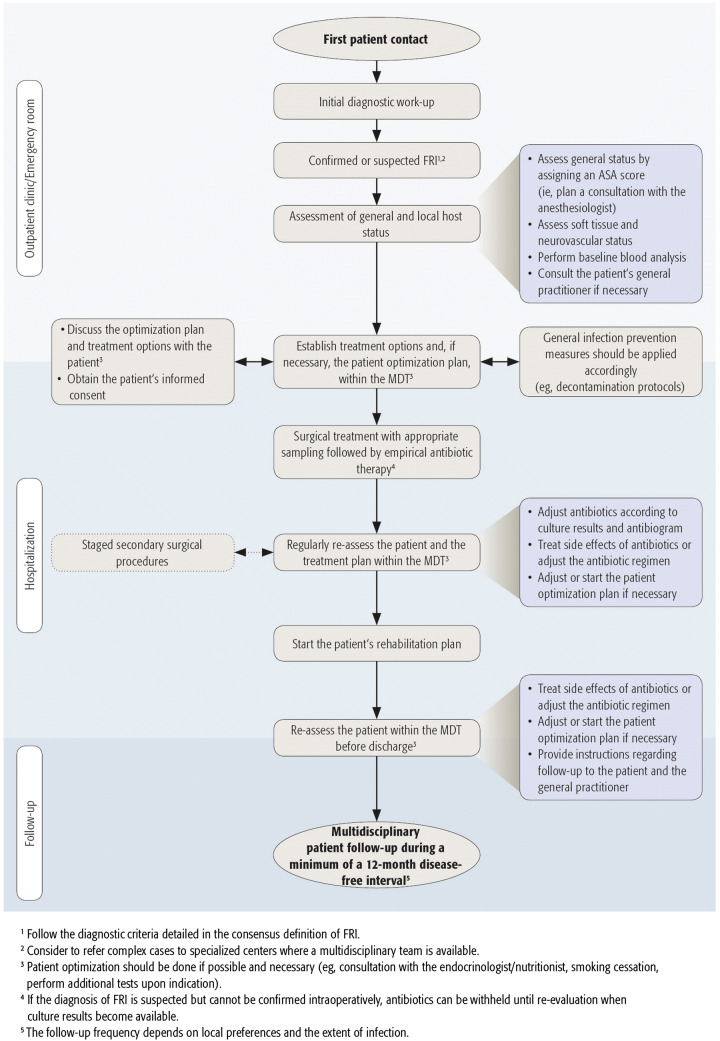
Fracture-related infection (FRI) remains a challenging complication that creates a heavy burden for orthopaedic trauma patients, their families and treating physicians, as well as for healthcare systems. Standardization of the diagnosis of FRI has been poor, which made the undertaking and comparison of studies difficult. Recently, a consensus definition based on diagnostic criteria for FRI was published. As a well-established diagnosis is the first step in the treatment process of FRI, such a definition should not only improve the quality of published reports but also daily clinical practice. The FRI consensus group recently developed guidelines to standardize treatment pathways and outcome measures. At the center of these recommendations was the implementation of a multidisciplinary team (MDT) approach. If such a team is not available, it is recommended to refer complex cases to specialized centers where a MDT is available and physicians are experienced with the treatment of FRI. This should lead to appropriate use of antimicrobials and standardization of surgical strategies. Furthermore, an MDT could play an important role in host optimization. Overall two main surgical concepts are considered, based on the fact that fracture fixation devices primarily target fracture consolidation and can be removed after healing, in contrast to periprosthetic joint infection were the implant is permanent. The first concept consists of implant retention and the second consists of implant removal (healed fracture) or implant exchange (unhealed fracture). In both cases, deep tissue sampling for microbiological examination is mandatory. Key aspects of the surgical management of FRI are a thorough debridement, irrigation with normal saline, fracture stability, dead space management and adequate soft tissue coverage. The use of local antimicrobials needs to be strongly considered. In case of FRI, empiric broad-spectrum antibiotic therapy should be started after tissue sampling. Thereafter, this needs to be adapted according to culture results as soon as possible. Finally, a minimum follow-up of 12 months after cessation of therapy is recommended. Standardized patient outcome measures purely focusing on FRI are currently not available but the patient-reported outcomes measurement information system (PROMIS) seems to be the preferred tool to assess the patients' short and long-term outcome. This review summarizes the current general principles which should be considered during the whole treatment process of patients with FRI based on recommendations from the FRI Consensus Group.Level of evidence: Level V.
Keywords: Diagnosis; Fracture; Fracture-related infection; Infection; Outcome; Treatment.
Conflict of interest statement
All authors declare no conflict of interest with respect to the preparation and writing of this article.
Figures
References
-
- Metsemakers WJ, Morgenstern M, McNally MA, Moriarty TF, McFadyen I, Scarborough M, Athanasou NA, Ochsner PE, Kuehl R, Raschke M, Borens O, Xie Z, Velkes S, Hungerer S, Kates SL, Zalavras C, Giannoudis PV, Richards RG, Verhofstad MHJ. Fracture-related infection: a consensus on definition from an international expert group. Injury. 2018;49(3):505–510. doi: 10.1016/j.injury.2017.08.040. - DOI - PubMed
-
- Govaert GAM, Kuehl R, Atkins BL, Trampuz A, Morgenstern M, Obremskey WT, Verhofstad MHJ, McNally MA, Metsemakers WJ, on behalfof the Fracture-Related Infection (FRI) Consensus Group Diagnosing fracture-related infection: current concepts and recommendations. J Orthop Trauma. 2019 doi: 10.1097/BOT.0000000000001614. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
