

Nonpharmacological Treatment of Army Service Members with Chronic Pain Is Associated with Fewer Adverse Outcomes After Transition to the Veterans Health Administration
- PMID: 31659663
- PMCID: PMC7080907
- DOI: 10.1007/s11606-019-05450-4
Nonpharmacological Treatment of Army Service Members with Chronic Pain Is Associated with Fewer Adverse Outcomes After Transition to the Veterans Health Administration
Abstract
Background: Potential protective effects of nonpharmacological treatments (NPT) against long-term pain-related adverse outcomes have not been examined.
Objective: To compare active duty U.S. Army service members with chronic pain who did/did not receive NPT in the Military Health System (MHS) and describe the association between receiving NPT and adverse outcomes after transitioning to the Veterans Health Administration (VHA).
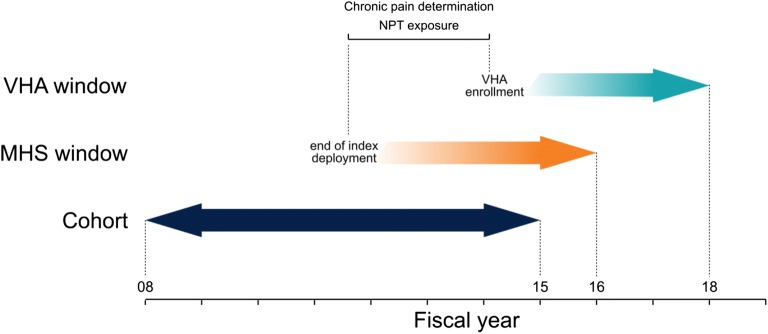
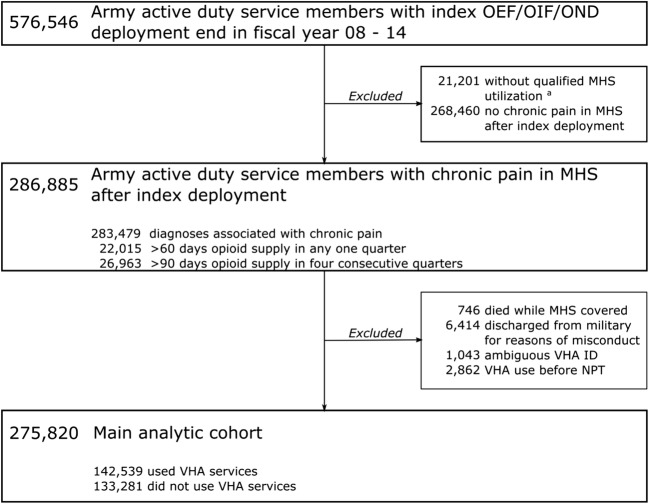
Design and participants: A longitudinal cohort study of active duty Army service members whose MHS healthcare records indicated presence of chronic pain after an index deployment to Iraq or Afghanistan in the years 2008-2014 (N = 142,539). Propensity score-weighted multivariable Cox proportional hazard models tested for differences in adverse outcomes between the NPT group and No-NPT group.
Exposures: NPT received in the MHS included acupuncture/dry needling, biofeedback, chiropractic care, massage, exercise therapy, cold laser therapy, osteopathic spinal manipulation, transcutaneous electrical nerve stimulation and other electrical manipulation, ultrasonography, superficial heat treatment, traction, and lumbar supports.
Main measures: Primary outcomes were propensity score-weighted proportional hazards for the following adverse outcomes: (a) diagnoses of alcohol and/or drug disorders; (b) poisoning with opioids, related narcotics, barbiturates, or sedatives; (c) suicide ideation; and (d) self-inflicted injuries including suicide attempts. Outcomes were determined based on ICD-9 and ICD-10 diagnoses recorded in VHA healthcare records from the start of utilization until fiscal year 2018.
Key results: The propensity score-weighted proportional hazards for the NPT group compared to the No-NPT group were 0.92 (95% CI 0.90-0.94, P < 0.001) for alcohol and/or drug use disorders; 0.65 (95% CI 0.51-0.83, P < 0.001) for accidental poisoning with opioids, related narcotics, barbiturates, or sedatives; 0.88 (95% CI 0.84-0.91, P < 0.001) for suicide ideation; and 0.83 (95% CI 0.77-0.90, P < 0.001) for self-inflicted injuries including suicide attempts.
Conclusions: NPT provided in the MHS to service members with chronic pain may reduce risk of long-term adverse outcomes.
Keywords: adverse outcomes; chronic pain; nonpharmacological treatment; opioids; veterans.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Institute of Medicine . Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: The National Academies Press; 2011. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
