

The Changing Epidemiology of HIV-Associated Adult Meningitis, Uganda 2015-2017
- PMID: 31660375
- PMCID: PMC6810358
- DOI: 10.1093/ofid/ofz419
The Changing Epidemiology of HIV-Associated Adult Meningitis, Uganda 2015-2017
Erratum in
-
Erratum to: The Changing Epidemiology of HIV-Associated Adult Meningitis, Uganda 2015-2017.Open Forum Infect Dis. 2019 Dec 3;6(12):ofz506. doi: 10.1093/ofid/ofz506. eCollection 2019 Dec. Open Forum Infect Dis. 2019. PMID: 31807608 Free PMC article.
Abstract
Background: Central nervous system (CNS) infections remain a major public health problem in Sub-Saharan Africa, causing 15%-25% of AIDS-related deaths. With widespread availability of antiretroviral therapy (ART) and the introduction of improved diagnostics, the epidemiology of infectious meningitis is evolving.
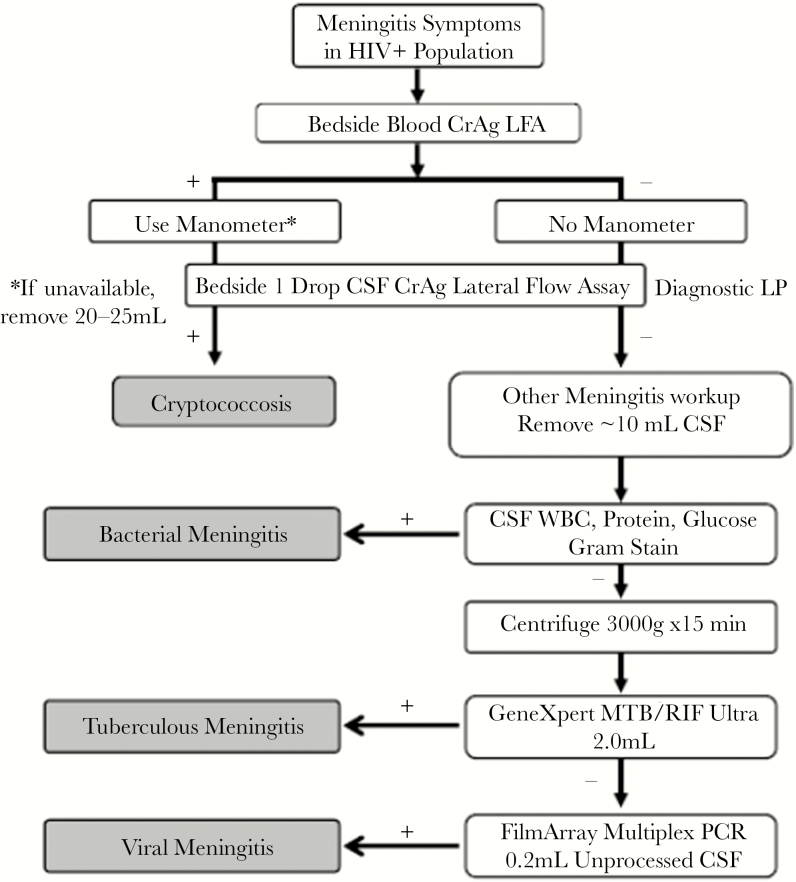
Methods: We prospectively enrolled adults presenting with HIV-associated meningitis in Kampala and Mbarara, Uganda, from March 2015 to September 2017. Participants had a structured, stepwise diagnostic algorithm performed of blood cryptococcal antigen (CrAg), CSF CrAg, Xpert MTB/RIF for tuberculous (TB) meningitis (TBM), Biofire multiplex polymerase chain reaction, and traditional microscopy and cultures.
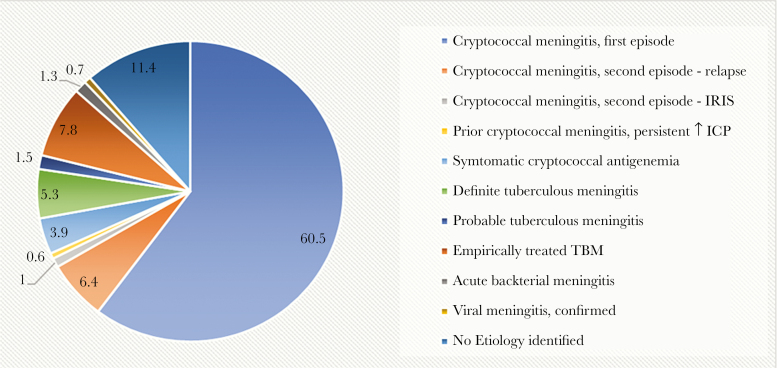
Results: We screened 842 consecutive adults with HIV presenting with suspected meningitis: 57% men, median age 35 years, median CD4 26 cells/mcL, and 55% presented on ART. Overall, 60.5% (509/842) were diagnosed with first-episode cryptococcal meningitis and 7.4% (62/842) with second episode. Definite/probable TB meningitis was the primary diagnosis in 6.9% (58/842); 5.3% (n = 45) had microbiologically confirmed (definite) TB meningitis. An additional 7.8% (66/842) did not meet the diagnostic threshold for definite/probable TBM but received empiric TBM therapy. Bacterial and viral meningitis were diagnosed in 1.3% (11/842) and 0.7% (6/842), respectively. The adoption of a cost-effective stepwise diagnostic algorithm allowed 79% (661/842) to have a confirmed microbiological diagnosis at an average cost of $44 per person.
Conclusions: Despite widespread ART availability, Cryptococcus remains the leading cause of HIV-associated meningitis. The second most common etiology was TB meningitis, treated in 14.7% overall. The increased proportion of microbiologically confirmed TBM cases reflects the impact of new improved molecular diagnostics.
Keywords: HIV/AIDS; bacterial meningitis; cryptococcal meningitis; tuberculous meningitis; viral meningitis.
© The Author(s) 2019. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- World Health Organization. Number of Suspected Meningitis Cases and Deaths Reported. Geneva: World Health Organization; 2015. Available at: http://www.who.int/gho/epidemic_diseases/meningitis/suspected_cases_deat.... Accessed 9 April 2018.
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
