

Outcome in juvenile idiopathic arthritis: a population-based study from Sweden
- PMID: 31661011
- PMCID: PMC6816211
- DOI: 10.1186/s13075-019-1994-8
Outcome in juvenile idiopathic arthritis: a population-based study from Sweden
Abstract
Background: As the treatment arsenal for children with juvenile idiopathic arthritis (JIA) has expanded during the last decades, follow-up studies are needed on children diagnosed in the era of biological treatment to evaluate if this has improved the outcome. Our aim was to study the epidemiology and outcome of JIA in southern Sweden using a population-based cohort of children with a validated diagnosis of JIA collected over 9 years.
Methods: Potential cases of JIA between 2002 and 2010 were collected after a database search, using the ICD codes M08-M09. The study area was Skåne, the southernmost county of Sweden (population 1.24 million; 17.6% aged < 16 years). The JIA diagnosis was validated and subcategorized through medical record review based on the criteria defined by the International League of Associations for Rheumatism (ILAR). Parameters on disease activity and pharmacologic treatment were recorded annually until the end of the study period (December 31, 2015).
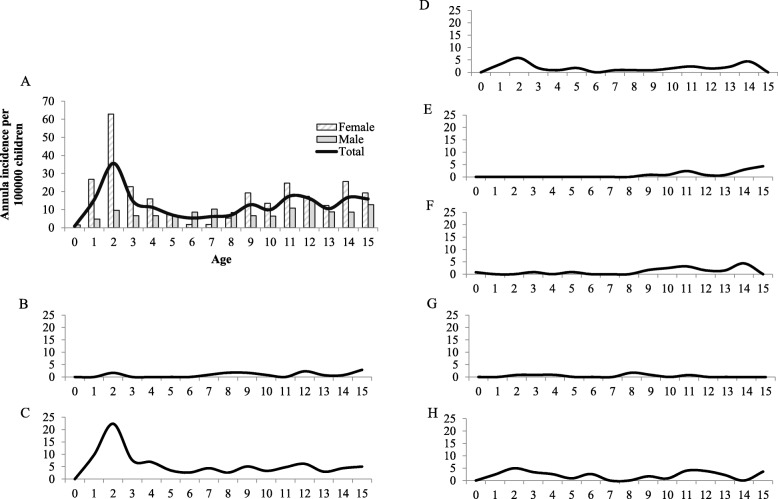
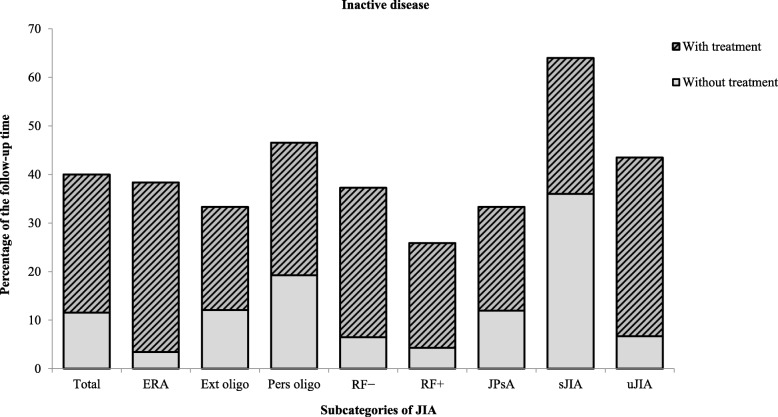
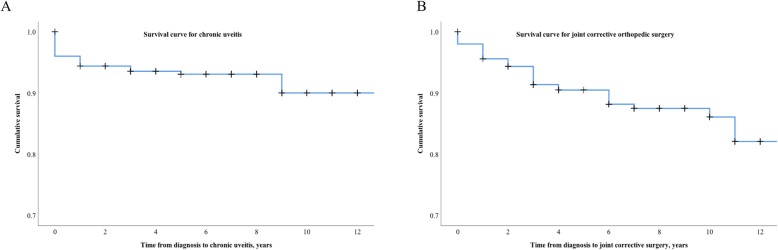
Results: In total, 251 cases of JIA were confirmed. The mean annual incidence rate for JIA was estimated to be 12.8/100,000 children < 16 years, with the highest age-specific annual incidence at the age of 2 years (36/100,000). Oligoarthritis was the largest subgroup (44.7%), and systemic JIA was the smallest subgroup (2.8%). Methotrexate was the most common disease-modifying anti-rheumatic drug prescribed (60.6%). Tumor necrosis factor alpha inhibitors were used as treatment for 23.9% of the children. Only 40.0% of the follow-up years, with a median follow-up time of 8 years, were free of arthritis or uveitis. Uveitis occurred in 10.8% of the children (8.0% chronic uveitis), and the need for joint corrective orthopedic surgery was 9.2%.
Conclusions: The incidence of JIA in this well-defined, population-based cohort is slightly lower than in previously published studies from Scandinavia. The need for orthopedic surgery and the presence of uveitis are diminished compared to studies with patients diagnosed more than 20 years ago. Children with JIA however still experience disease activity more than 50% of the time. In conclusion, we still have long-term challenges in the care for children with JIA, in spite of state-of-the-art treatment.
Keywords: Follow-up; Incidence; JIA; Outcome; Population-based; Uveitis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Brewer EJ, Jr, Bass J, Baum J, Cassidy JT, Fink C, Jacobs J, et al. Current proposed revision of JRA criteria. JRA Criteria Subcommittee of the Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Section of the Arthritis Foundation. Arthritis Rheum. 1977;20(2 Suppl):195–199. - PubMed
-
- PH W. Special meeting on: nomenclature and classification of arthritis in children. In: Munthe E, editor. The care of rheumatic children, EULAR; Basel 1978. p. 47–50.
-
- Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390–392. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
