

Role of community-based active case finding in screening tuberculosis in Yunnan province of China
- PMID: 31661031
- PMCID: PMC6819334
- DOI: 10.1186/s40249-019-0602-0
Role of community-based active case finding in screening tuberculosis in Yunnan province of China
Erratum in
-
Correction to: Role of community-based active case finding in screening tuberculosis in Yunnan province of China.Infect Dis Poverty. 2020 Jan 18;9(1):7. doi: 10.1186/s40249-020-0625-6. Infect Dis Poverty. 2020. PMID: 31954401 Free PMC article.
Abstract
Background: The barriers to access diagnosis and receive treatment, in addition to insufficient case identification and reporting, lead to tuberculosis (TB) spreads in communities, especially among hard-to-reach populations. This study evaluated a community-based active case finding (ACF) strategy for the detection of tuberculosis cases among high-risk groups and general population in China between 2013 and 2015.
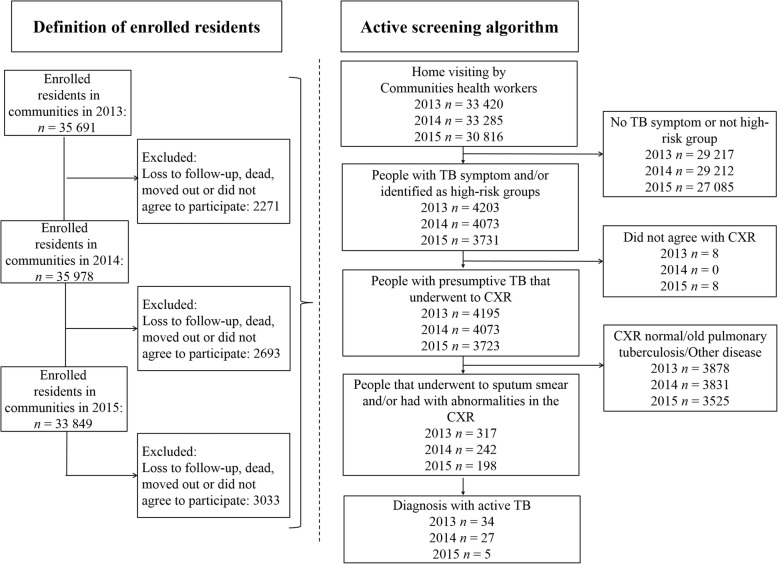
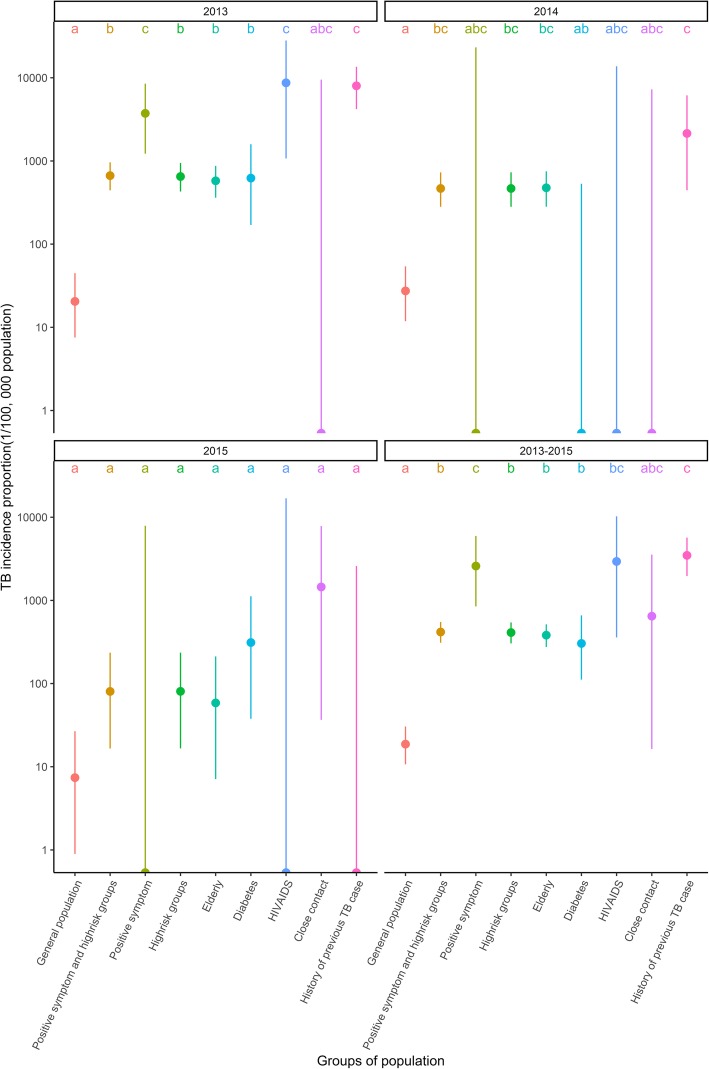
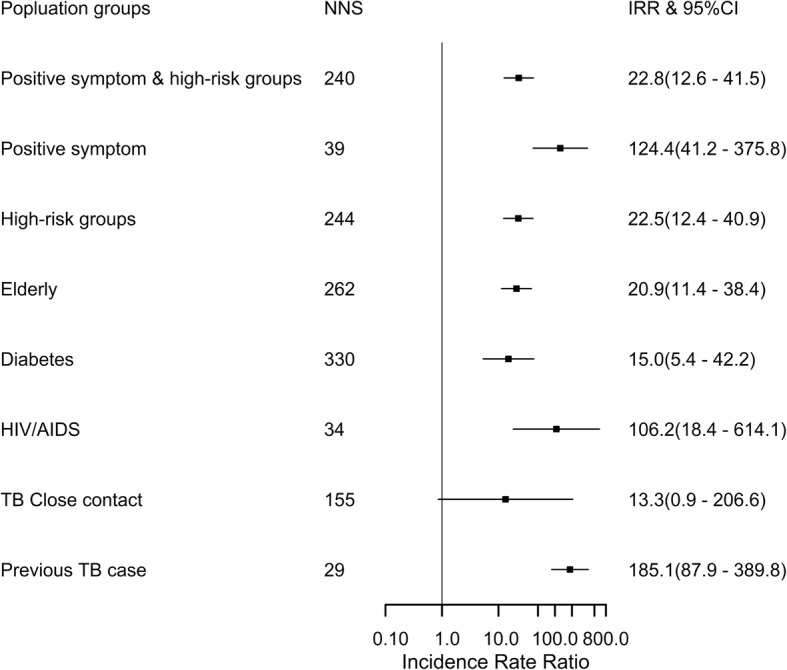
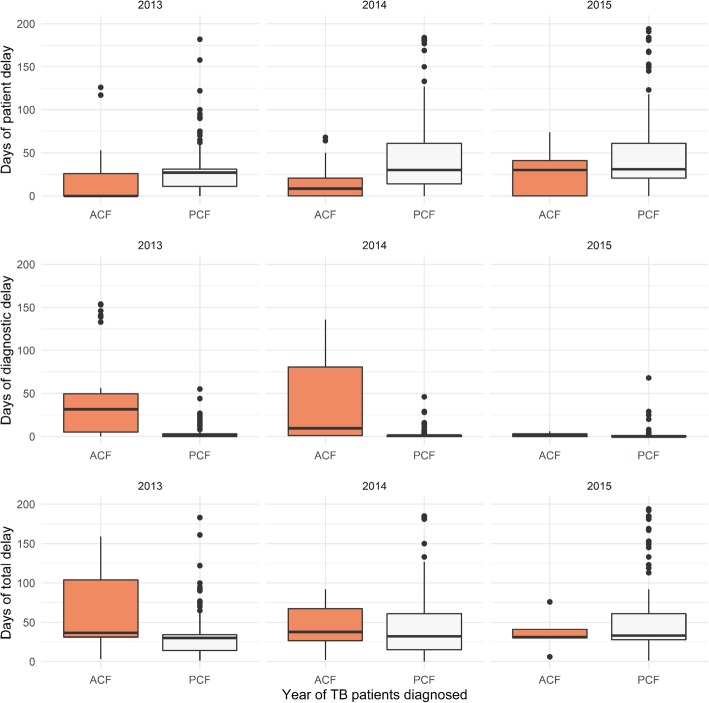
Methods: This retrospective cohort study conducted an ACF in ten communities of Dongchuan County, located in northeast Yunnan Province between 2013 and 2015; and compared to 136 communities that had passive case finding (PCF). The algorithm for ACF was: 1) screen for TB symptoms among community enrolled residents by home visits, 2) those with positive symptoms along with defined high-risk groups underwent chest X-ray (CXR), followed by sputum microscopy confirmation. TB incidence proportion and the number needed to screen (NNS) to detect one case were calculated to evaluate the ACF strategy compared to PCF, chi-square test was applied to compare the incidence proportion of TB cases' demography and the characteristics for detected cases under different strategies. Thereafter, the incidence rate ratio (IRR) and multiple Fisher's exact test were applied to compare the incidence proportion between general population and high-risk groups. Patient and diagnostic delays for ACF and PCF were compared by Wilcoxon rank sum test.
Results: A total of 97 521 enrolled residents were visited with the ACF cumulatively, 12.3% were defined as high-risk groups or had TB symptoms. Sixty-six new TB patients were detected by ACF. There was no significant difference between the cumulative TB incidence proportion for ACF (67.7/100000 population) and the prevalence for PCF (62.6/100000 population) during 2013 to 2015, though the incidence proportion in ACF communities decreased after three rounds active screening, concurrent with the remained stable prevalence in PCF communities. The cumulative NNS were 34, 39 and 29 in HIV/AIDS infected individuals, people with positive TB symptoms and history of previous TB, respectively, compared to 1478 in the general population. The median patient delay under ACF was 1 day (Interquartile range, IQR: 0-27) compared to PCF with 30 days (IQR: 14-61).
Conclusions: This study confirmed that massive ACF was not effective in general population in a moderate TB prevalence setting. The priority should be the definition and targeting of high-risk groups in the community before the screening process is launched. The shorter time interval of ACF between TB symptoms onset and linkage to healthcare service may decrease the risk of TB community transmission. Furthermore, integrated ACF strategy in the National Project of Basic Public Health Service may have long term public health impact.
Keywords: Active case finding; Diagnosis; Passive case finding; Patient delay; Tuberculosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization . Global Tuberculosis Report 2018. Geneva: World Health Organization; 2018.
-
- World Health Organization. WHO End TB Strategy. 2015. http://www.who.int/tb/post2015_strategy/en/. Accessed 11 Jul 2018.
-
- United Nations Development Programme . Sustainable development goals. 2012.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
