

Volatile anesthetics versus total intravenous anesthesia in patients undergoing coronary artery bypass grafting: An updated meta-analysis and trial sequential analysis of randomized controlled trials
- PMID: 31661512
- PMCID: PMC6818786
- DOI: 10.1371/journal.pone.0224562
Volatile anesthetics versus total intravenous anesthesia in patients undergoing coronary artery bypass grafting: An updated meta-analysis and trial sequential analysis of randomized controlled trials
Abstract
Background: The benefits of volatile anesthetics in coronary artery bypass grafting (CABG) patients remain controversial. We aimed to conduct an updated meta-analysis to assess whether the use of volatile anesthetics during CABG could reduce mortality and other outcomes.
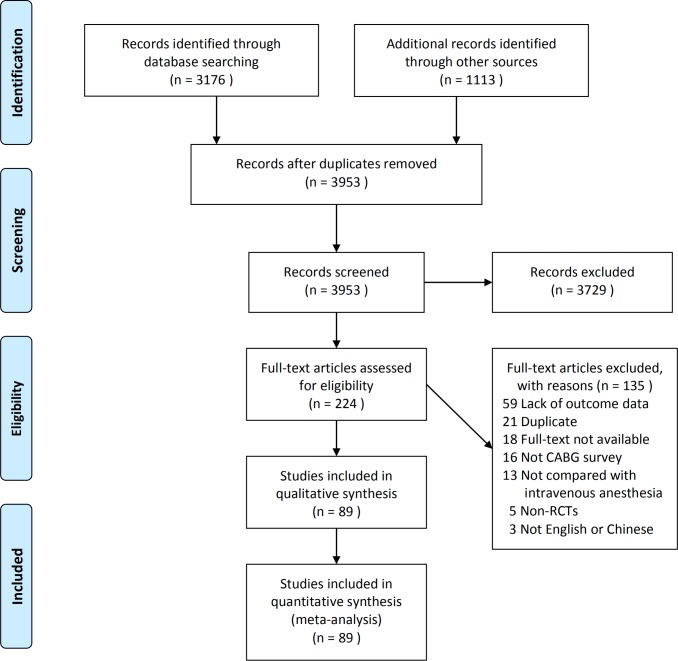
Methods: We searched eight databases from inception to June 2019 and included randomized controlled trials (RCTs) comparing the effects of volatile anesthetics versus total intravenous anesthesia (TIVA) in CABG patients. The primary outcomes were operative mortality and one-year mortality. The secondary outcomes included the length of stay in the intensive care unit (ICU) and hospital and postoperative safety outcomes (myocardial infarction, heart failure, arrhythmia, stroke, delirium, postoperative cognitive impairment, acute kidney injury, and the use of intra-aortic balloon pump (IABP) or other mechanical circulatory support). Trial sequential analysis (TSA) was performed to control for random errors.
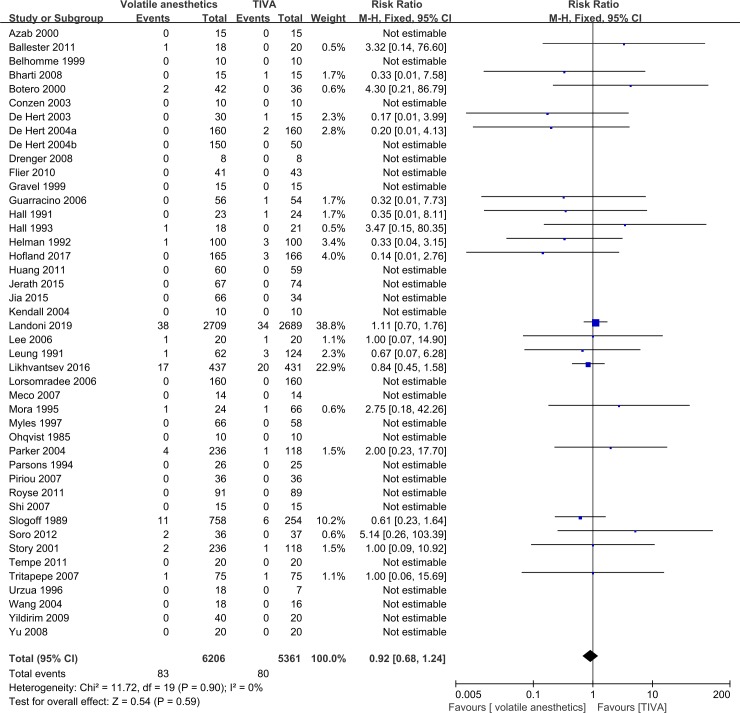
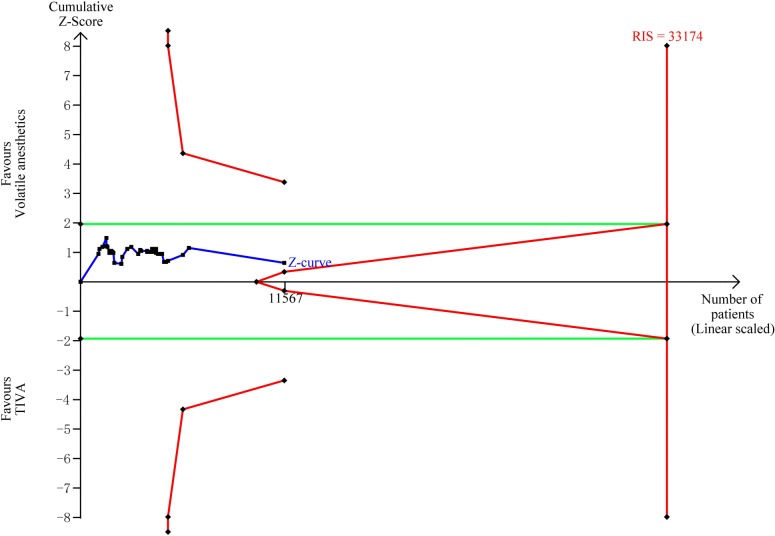
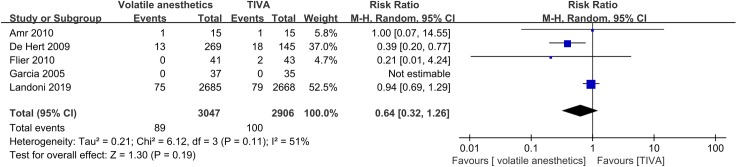
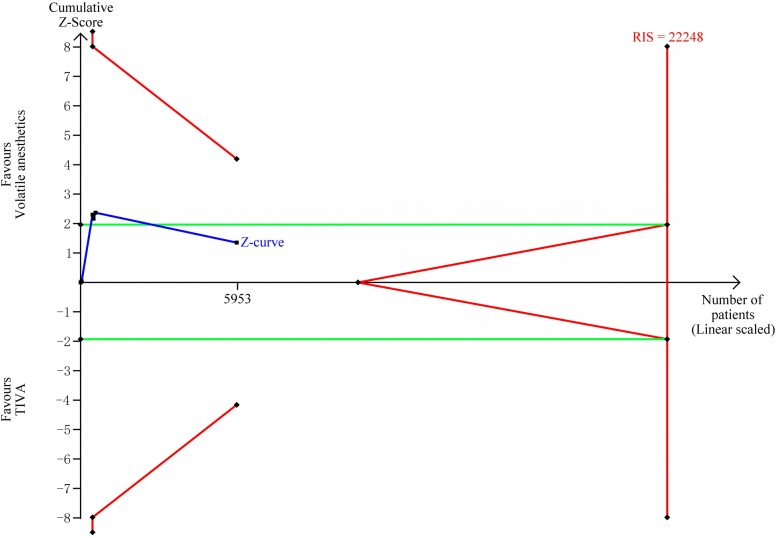
Results: A total of 89 RCTs comprising 14,387 patients were included. There were no significant differences between the volatile anesthetics and TIVA groups in operative mortality (relative risk (RR) = 0.92, 95% confidence interval (CI): 0.68-1.24, p = 0.59, I2 = 0%), one-year mortality (RR = 0.64, 95% CI: 0.32-1.26, p = 0.19, I2 = 51%), or any of the postoperative safety outcomes. The lengths of stay in the ICU and hospital were shorter in the volatile anesthetics group than in the TIVA group. TSA revealed that the results for operative mortality, one-year mortality, length of stay in the ICU, heart failure, stroke, and the use of IABP were inconclusive.
Conclusions: Conventional meta-analysis suggests that the use of volatile anesthetics during CABG is not associated with reduced risk of mortality or other postoperative safety outcomes when compared with TIVA. TSA shows that the current evidence is insufficient and inconclusive. Thus, future large RCTs are required to clarify this issue.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Effect of volatile anesthetics on mortality and clinical outcomes in patients undergoing coronary artery bypass grafting: a meta-analysis of randomized clinical trials.Minerva Anestesiol. 2020 Oct;86(10):1065-1078. doi: 10.23736/S0375-9393.20.14304-9. Epub 2020 Mar 11. Minerva Anestesiol. 2020. PMID: 32162897
-
Sevoflurane Versus Total Intravenous Anesthesia for Isolated Coronary Artery Bypass Surgery With Cardiopulmonary Bypass: A Randomized Trial.J Cardiothorac Vasc Anesth. 2016 Oct;30(5):1221-7. doi: 10.1053/j.jvca.2016.02.030. Epub 2016 Mar 3. J Cardiothorac Vasc Anesth. 2016. PMID: 27431595 Clinical Trial.
-
Volatile Versus Total Intravenous Anesthesia on Postoperative Delirium in Adult Patients Undergoing Cardiac Valve Surgery: A Randomized Clinical Trial.Anesth Analg. 2023 Jan 1;136(1):60-69. doi: 10.1213/ANE.0000000000006257. Epub 2022 Oct 27. Anesth Analg. 2023. PMID: 36301724 Clinical Trial.
-
Inhalation versus intravenous anesthesia for adults undergoing heart valve surgery: a systematic review and meta-analysis.Minerva Anestesiol. 2019 Jun;85(6):665-675. doi: 10.23736/S0375-9393.19.13377-9. Epub 2019 Feb 13. Minerva Anestesiol. 2019. PMID: 30762324
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
Cited by
-
The effects of volatile anesthetics and propofol in patients undergoing off-pump coronary artery bypass grafting: a systematic review and meta-analysis.Front Cardiovasc Med. 2023 Nov 15;10:1271557. doi: 10.3389/fcvm.2023.1271557. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 38034375 Free PMC article. Review.
-
Molecular Aspects of Volatile Anesthetic-Induced Organ Protection and Its Potential in Kidney Transplantation.Int J Mol Sci. 2021 Mar 8;22(5):2727. doi: 10.3390/ijms22052727. Int J Mol Sci. 2021. PMID: 33800423 Free PMC article. Review.
-
Inhaled Anesthetics: Environmental Role, Occupational Risk, and Clinical Use.J Clin Med. 2021 Mar 22;10(6):1306. doi: 10.3390/jcm10061306. J Clin Med. 2021. PMID: 33810063 Free PMC article. Review.
-
Prophylactic effect of intravenous lidocaine against cognitive deficit after cardiac surgery: A PRISMA-compliant meta-analysis and trial sequential analysis.Medicine (Baltimore). 2022 Sep 2;101(35):e30476. doi: 10.1097/MD.0000000000030476. Medicine (Baltimore). 2022. PMID: 36107567 Free PMC article.
-
Volatile Anaesthesia versus Total Intravenous Anaesthesia for Cardiac Surgery-A Narrative Review.J Clin Med. 2022 Oct 13;11(20):6031. doi: 10.3390/jcm11206031. J Clin Med. 2022. PMID: 36294353 Free PMC article. Review.
References
-
- Alexander JH, Smith PK. Coronary-Artery Bypass Grafting. N Engl J Med. 2016;375(10):e22. - PubMed
-
- Moazzami K, Dolmatova E, Maher J, Gerula C, Sambol J, Klapholz M, et al. In-Hospital Outcomes and Complications of Coronary Artery Bypass Grafting in the United States Between 2008 and 2012. Journal of cardiothoracic and vascular anesthesia. 2017;31(1):19–25. 10.1053/j.jvca.2016.08.008 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
