

PD-L1/PD-1 Axis in Glioblastoma Multiforme
- PMID: 31661771
- PMCID: PMC6862444
- DOI: 10.3390/ijms20215347
PD-L1/PD-1 Axis in Glioblastoma Multiforme
Abstract
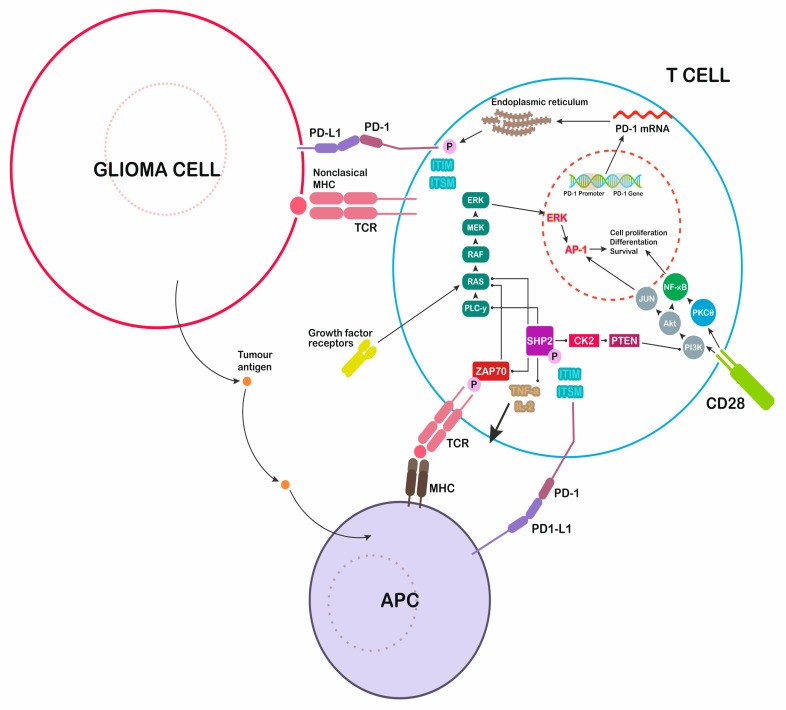
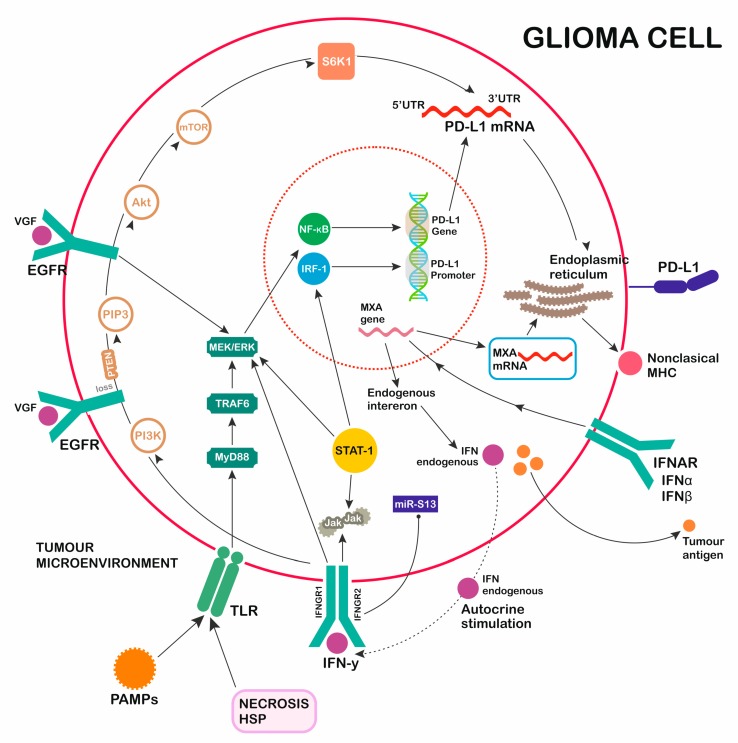
Glioblastoma (GBM) is the most popular primary central nervous system cancer and has an extremely expansive course. Aggressive tumor growth correlates with short median overall survival (OS) oscillating between 14 and 17 months. The survival rate of patients in a three-year follow up oscillates around 10%. The interaction of the proteins programmed death-1 (PD-1) and programmed cell death ligand (PD-L1) creates an immunoregulatory axis promoting invasion of glioblastoma multiforme cells in the brain tissue. The PD-1 pathway maintains immunological homeostasis and protects against autoimmunity. PD-L1 expression on glioblastoma surface promotes PD-1 receptor activation in microglia, resulting in the negative regulation of T cell responses. Glioblastoma multiforme cells induce PD-L1 secretion by activation of various receptors such as toll like receptor (TLR), epidermal growth factor receptor (EGFR), interferon alpha receptor (IFNAR), interferon-gamma receptor (IFNGR). Binding of the PD-1 ligand to the PD-1 receptor activates the protein tyrosine phosphatase SHP-2, which dephosphorylates Zap 70, and this inhibits T cell proliferation and downregulates lymphocyte cytotoxic activity. Relevant studies demonstrated that the expression of PD-L1 in glioma correlates with WHO grading and could be considered as a tumor biomarker. Studies in preclinical GBM mouse models confirmed the safety and efficiency of monoclonal antibodies targeting the PD-1/PD-L1 axis. Satisfactory results such as significant regression of tumor mass and longer animal survival time were observed. Monoclonal antibodies inhibiting PD-1 and PD-L1 are being tested in clinical trials concerning patients with recurrent glioblastoma multiforme.
Keywords: GBM; PD1; PD1 ligand; glioblastoma multiforme.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Greer L., Pannullo S.C., Smith A.W., Taube S., Yondorf M.Z., Parashar B., Trichter S., Nedialkova L., Sabbas A., Christos P., et al. Accelerated hypofractionated radiotherapy in the era of concurrent temozolomide chemotherapy in elderly patients with glioblastoma multiforme. Cureus. 2017;9:e1388. doi: 10.7759/cureus.1388. - DOI - PMC - PubMed
-
- Fernandes C., Costa A., Osório L., Lago R.C., Linhares P., Carvalho B., Caeiro C. Current standards of care in glioblastoma therapy. In: De Vleeschouwer S., editor. Glioblastoma [Internet] Codon Publications; Brisbane, Australia: 2007. Chapter 11. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
