

Microvascular Obstruction in ST-Segment Elevation Myocardial Infarction: Looking Back to Move Forward. Focus on CMR
- PMID: 31661823
- PMCID: PMC6912395
- DOI: 10.3390/jcm8111805
Microvascular Obstruction in ST-Segment Elevation Myocardial Infarction: Looking Back to Move Forward. Focus on CMR
Abstract
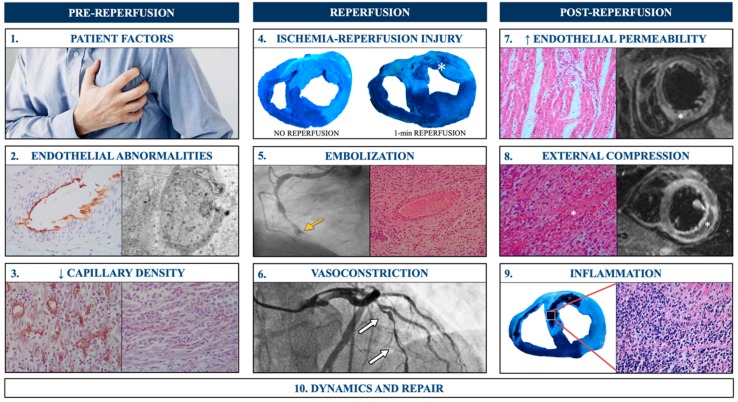
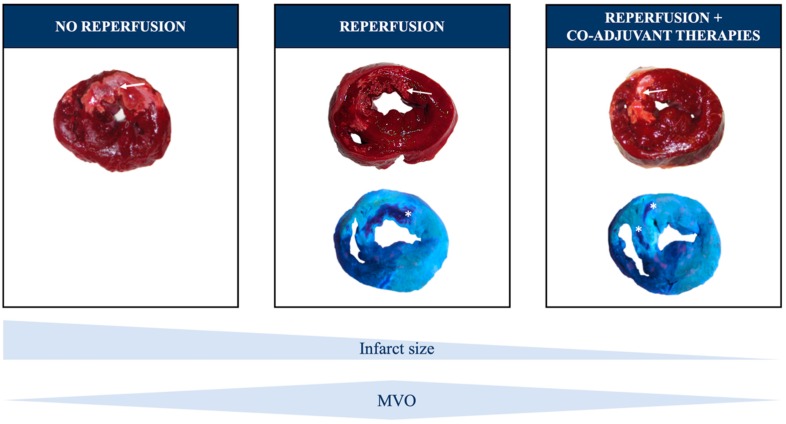
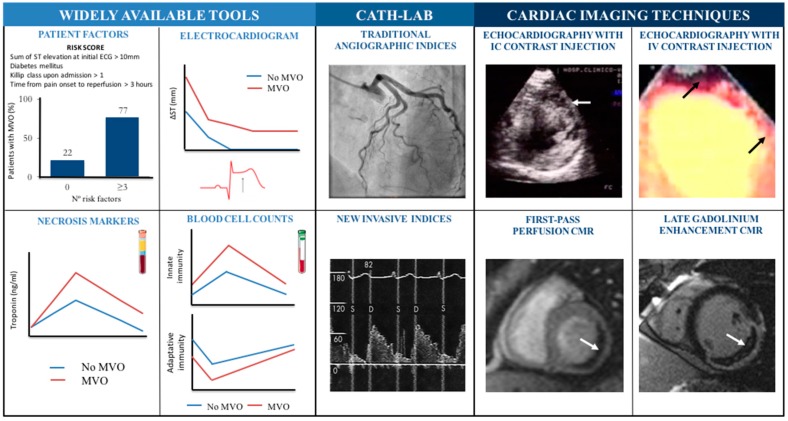
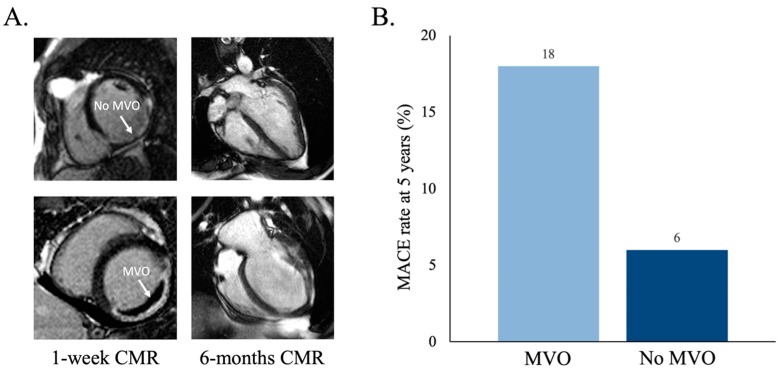
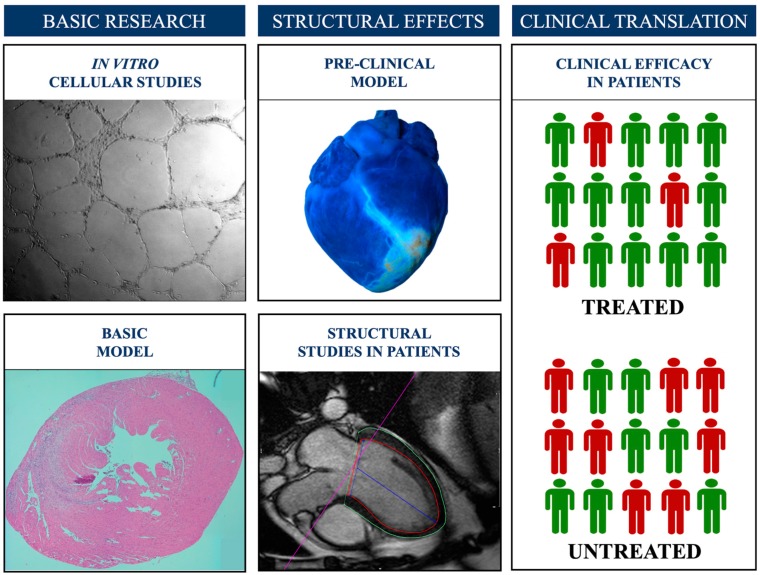
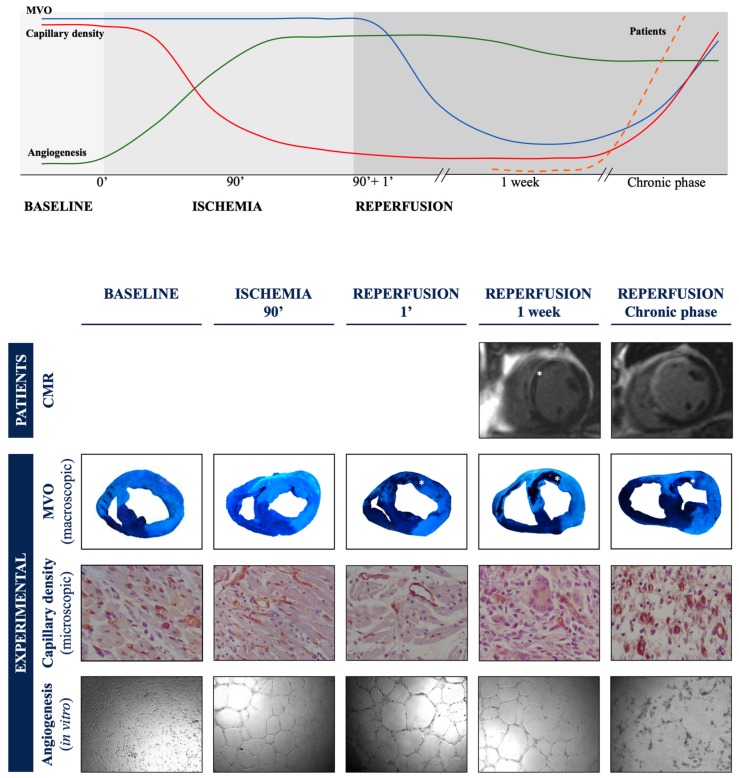
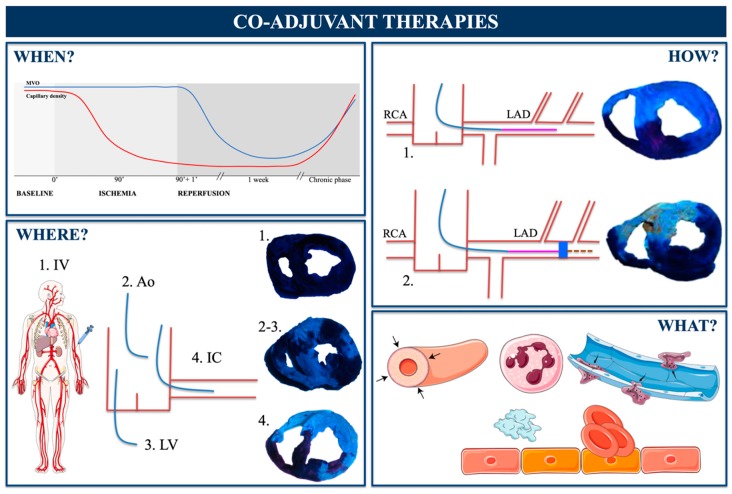
After a myocardial infarction (MI), despite the resolution of the coronary occlusion, the deterioration of myocardial perfusion persists in a considerable number of patients. This phenomenon is known as microvascular obstruction (MVO). Initially, the focus was placed on re-establishing blood flow in the epicardial artery. Then, the observation that MVO has profound negative structural and prognostic repercussions revived interest in microcirculation. In the near future, the availability of co-adjuvant therapies (beyond timely coronary reperfusion) aimed at preventing, minimizing, and repairing MVOs and finding convincing answers to questions regarding what, when, how, and where to administer these therapies will be of utmost importance. The objective of this work is to review the state-of-the-art concepts on pathophysiology, diagnostic methods, and structural and clinical implications of MVOs in patients with ST-segment elevation MIs. Based on this knowledge we discuss previously-tested and future opportunities for the prevention and repair of MVO.
Keywords: microvascular obstruction; myocardial infarction; reperfusion injury.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
Dynamic Changes in ST Segment Resolution After Myocardial Infarction and the Association with Microvascular Injury on Cardiac Magnetic Resonance Imaging.Heart Lung Circ. 2011 Feb;20(2):111-8. doi: 10.1016/j.hlc.2010.09.006. Epub 2010 Oct 12. Heart Lung Circ. 2011. PMID: 20943440
-
Prediction of microvascular obstruction by coronary artery angiography score after acute ST-segment elevation myocardial infarction: a single-center retrospective observational study.BMC Cardiovasc Disord. 2022 Sep 14;22(1):410. doi: 10.1186/s12872-022-02836-x. BMC Cardiovasc Disord. 2022. PMID: 36104684 Free PMC article.
-
Cardiac magnetic resonance derived late microvascular obstruction assessment post ST-segment elevation myocardial infarction is the best predictor of left ventricular function: a comparison of angiographic and cardiac magnetic resonance derived measurements.Int J Cardiovasc Imaging. 2012 Dec;28(8):1971-81. doi: 10.1007/s10554-012-0021-9. Epub 2012 Feb 5. Int J Cardiovasc Imaging. 2012. PMID: 22310980
-
Optimized Treatment of ST-Elevation Myocardial Infarction.Circ Res. 2019 Jul 5;125(2):245-258. doi: 10.1161/CIRCRESAHA.119.315344. Epub 2019 Jul 3. Circ Res. 2019. PMID: 31268854 Review.
-
Predictors of Microvascular Reperfusion After Myocardial Infarction.Curr Cardiol Rep. 2021 Feb 23;23(3):21. doi: 10.1007/s11886-021-01442-1. Curr Cardiol Rep. 2021. PMID: 33624185 Free PMC article. Review.
Cited by
-
Melatonin: a promising neuroprotective agent for cerebral ischemia-reperfusion injury.Front Aging Neurosci. 2023 Aug 4;15:1227513. doi: 10.3389/fnagi.2023.1227513. eCollection 2023. Front Aging Neurosci. 2023. PMID: 37600520 Free PMC article. Review.
-
Remifentanil pretreatment ameliorates H/R-induced cardiac microvascular endothelial cell dysfunction by regulating the PI3K/Akt/HIF-1α signaling pathway.Bioengineered. 2021 Dec;12(1):7872-7881. doi: 10.1080/21655979.2021.1969843. Bioengineered. 2021. PMID: 34612779 Free PMC article.
-
[A cardiac magnetic resonance-based risk prediction model for left ventricular adverse remodeling following percutaneous coronary intervention for acute ST-segment elevation myocardial infarction: a multi-center prospective study].Nan Fang Yi Ke Da Xue Xue Bao. 2025 Apr 20;45(4):669-683. doi: 10.12122/j.issn.1673-4254.2025.04.01. Nan Fang Yi Ke Da Xue Xue Bao. 2025. PMID: 40294916 Free PMC article. Chinese.
-
Invasive Evaluation of the Microvasculature in Acute Myocardial Infarction: Coronary Flow Reserve versus the Index of Microcirculatory Resistance.J Clin Med. 2019 Dec 29;9(1):86. doi: 10.3390/jcm9010086. J Clin Med. 2019. PMID: 31905738 Free PMC article. Review.
-
Role of Cardiac Magnetic Resonance to Improve Risk Prediction Following Acute ST-Elevation Myocardial Infarction.J Clin Med. 2020 Apr 7;9(4):1041. doi: 10.3390/jcm9041041. J Clin Med. 2020. PMID: 32272692 Free PMC article. Review.
References
-
- Hamirani Y.S., Wong A., Kramer C.M., Salerno M. Effect of microvascular obstruction and intramyocardial hemorrhage by CMR on LV remodeling and outcomes after myocardial infarction: A systematic review and meta-analysis. JACC Cardiovasc. Imaging. 2014;7:940–952. doi: 10.1016/j.jcmg.2014.06.012. - DOI - PMC - PubMed
-
- Gavara J., Rodriguez-Palomares J.F., Valente F., Monmeneu J.V., Lopez-Lereu M.P., Bonanad C., Ferreira-Gonzalez I., Garcia del Blanco B., Rodriguez-Garcia J., Mutuberria M., et al. Prognostic value of strain by tissue tracking cardiac magnetic resonance after ST-segment elevation myocardial infarction. JACC Cardiovasc. Imaging. 2018;11:1448–1457. doi: 10.1016/j.jcmg.2017.09.017. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
