

Effect of anti-C5 antibody on recuperation from ischemia/reperfusion-induced acute kidney injury
- PMID: 31662004
- PMCID: PMC6830203
- DOI: 10.1080/0886022X.2019.1677248
Effect of anti-C5 antibody on recuperation from ischemia/reperfusion-induced acute kidney injury
Abstract
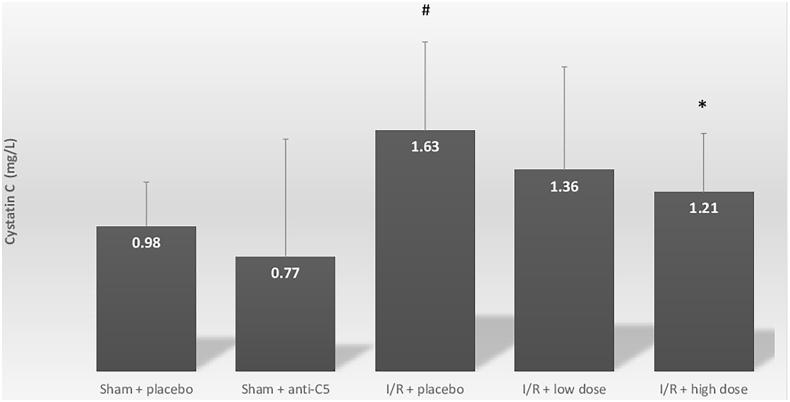
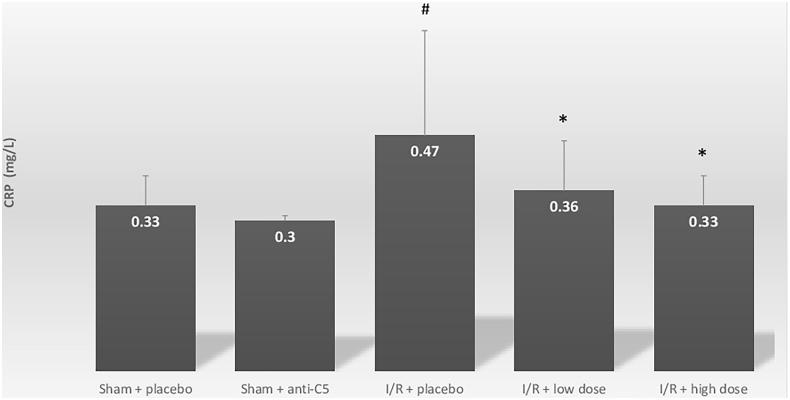
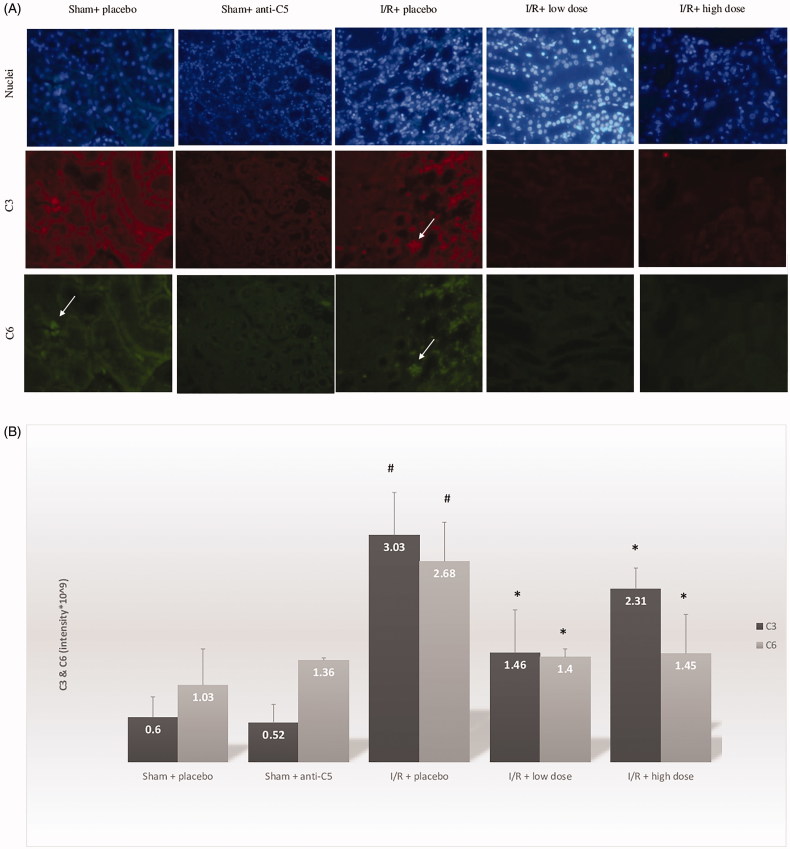
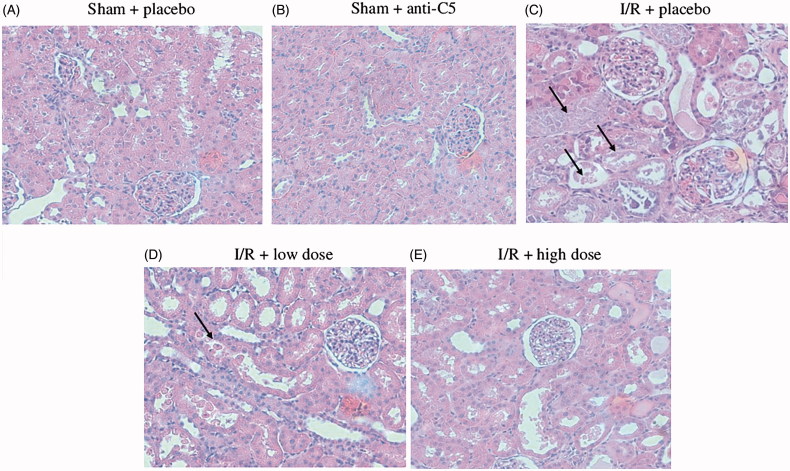
AbstractAim: The complement system is activated in acute kidney injury (AKI). Anti-C5 antibody targets the common terminal portion of the complement cascade that generate the terminal complex C5b-9 and has a renal-protective effect in paroxysmal nocturnal hemoglobinuria. However, the anti-C5 antibody's role in ischemia/reperfusion (I/R)-induced AKI has not been fully investigated. We therefore evaluated its effect on the pathophysiological cascade of I/R-induced AKI.Methods: Sprague-Dawley rats underwent unilateral right kidney nephrectomies with simultaneous clamping of the contralateral hilum for 60 min (ischemia), followed by reperfusion. In addition to a placebo, two treatment groups received either high or low doses of anti-C5 monoclonal antibody. After 48 h, the rats were euthanized, blood was drawn to evaluate systemic inflammation and to estimate glomerular filtration rate (GFR). The remaining kidney was removed for pathological evaluation and intra-renal complement activation.Results: I/R induced significant intra-renal complement activation and systemic inflammation compared with unilateral nephrectomy group. The anti-C5 antibody ameliorated the intra-renal complement activation (intra-renal C3 and C6), reduced systemic inflammation (C-reactive protein, and systemic C3), decreased intra-renal acute tubular necrosis damage and improved GFR (seen by the sensitive marker, serum cystatin C; 1.63 mg/L (I/R + placebo), 1.36 mg/L (I/R + low dose) and 1.21 mg/L (I/R + high dose), p = .08 and .03 compared with I/R + placebo).Conclusion: In I/R-induced AKI, the monoclonal anti-C5 complement factor ameliorates intra renal complement activation, decreases local and systemic inflammation and may improve GFR.
Keywords: Acute kidney injury; C5-antibody; complement system; ischemia-reperfusion injury; rat model.
Figures
Similar articles
-
Inhibition of complement factor C5 protects against renal ischemia-reperfusion injury: inhibition of late apoptosis and inflammation.Transplantation. 2003 Feb 15;75(3):375-82. doi: 10.1097/01.TP.0000044455.05584.2A. Transplantation. 2003. PMID: 12589162
-
Human mesenchymal stromal cells ameliorate complement induced inflammatory cascade and improve renal functions in a rat model of ischemia-reperfusion induced acute kidney injury.PLoS One. 2019 Sep 12;14(9):e0222354. doi: 10.1371/journal.pone.0222354. eCollection 2019. PLoS One. 2019. PMID: 31513644 Free PMC article.
-
Effect of captopril treatment on recuperation from ischemia/reperfusion-induced acute renal injury.Nephrol Dial Transplant. 2012 Jan;27(1):136-45. doi: 10.1093/ndt/gfr256. Epub 2011 Jun 16. Nephrol Dial Transplant. 2012. PMID: 21680852
-
Inflammaging and Complement System: A Link Between Acute Kidney Injury and Chronic Graft Damage.Front Immunol. 2020 May 7;11:734. doi: 10.3389/fimmu.2020.00734. eCollection 2020. Front Immunol. 2020. PMID: 32457738 Free PMC article. Review.
-
The role of the complement system in acute kidney injury.Semin Nephrol. 2013 Nov;33(6):543-56. doi: 10.1016/j.semnephrol.2013.08.005. Semin Nephrol. 2013. PMID: 24161039 Free PMC article. Review.
Cited by
-
Be aware of acute kidney injury in critically ill children with COVID-19.Pediatr Nephrol. 2021 Jan;36(1):163-169. doi: 10.1007/s00467-020-04715-z. Epub 2020 Aug 26. Pediatr Nephrol. 2021. PMID: 32844290 Free PMC article.
-
Recent advances in nanotherapeutics for the treatment and prevention of acute kidney injury.Asian J Pharm Sci. 2021 Jul;16(4):432-443. doi: 10.1016/j.ajps.2020.11.001. Epub 2020 Nov 27. Asian J Pharm Sci. 2021. PMID: 34703493 Free PMC article. Review.
-
The case of complement activation in COVID-19 multiorgan impact.Kidney Int. 2020 Aug;98(2):314-322. doi: 10.1016/j.kint.2020.05.013. Epub 2020 May 24. Kidney Int. 2020. PMID: 32461141 Free PMC article. Review.
-
Inflammatory stress in SARS-COV-2 associated Acute Kidney Injury.Int J Biol Sci. 2021 Apr 10;17(6):1497-1506. doi: 10.7150/ijbs.58791. eCollection 2021. Int J Biol Sci. 2021. PMID: 33907513 Free PMC article. Review.
-
Insights into Repeated Renal Injury Using RNA-Seq with Two New RPTEC Cell Lines.Int J Mol Sci. 2023 Sep 18;24(18):14228. doi: 10.3390/ijms241814228. Int J Mol Sci. 2023. PMID: 37762531 Free PMC article.
References
-
- Chawla LS, Kimmel PL. Acute kidney injury and chronic kidney disease: an integrated clinical syndrome. Kidney Int. 2012;82(5):516–524. - PubMed
-
- Hoste EA, Kellum JA. Incidence, classification, and outcomes of acute kidney injury. Contrib Nephrol. 2007;156:32–38. - PubMed
-
- Singbartl K, Kellum JA. AKI in the ICU: definition, epidemiology, risk stratification, and outcomes. Kidney Int. 2012;81(9):819–825. - PubMed
-
- Chan RK, Ibrahim SI, Verna N, et al. . Ischaemia-reperfusion is an event triggered by immune complexes and complement. Br J Surg. 2003;90(12):1470–1478. - PubMed
-
- Thadhani R, Pascual M, Bonventre JV. Acute renal failure. N Engl J Med. 1996;334(22):1448–1460. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous