

A Clinical Pathway to Standardize Care of Children With Delirium in Pediatric Inpatient Settings
- PMID: 31662421
- PMCID: PMC11416144
- DOI: 10.1542/hpeds.2019-0115
A Clinical Pathway to Standardize Care of Children With Delirium in Pediatric Inpatient Settings
Abstract
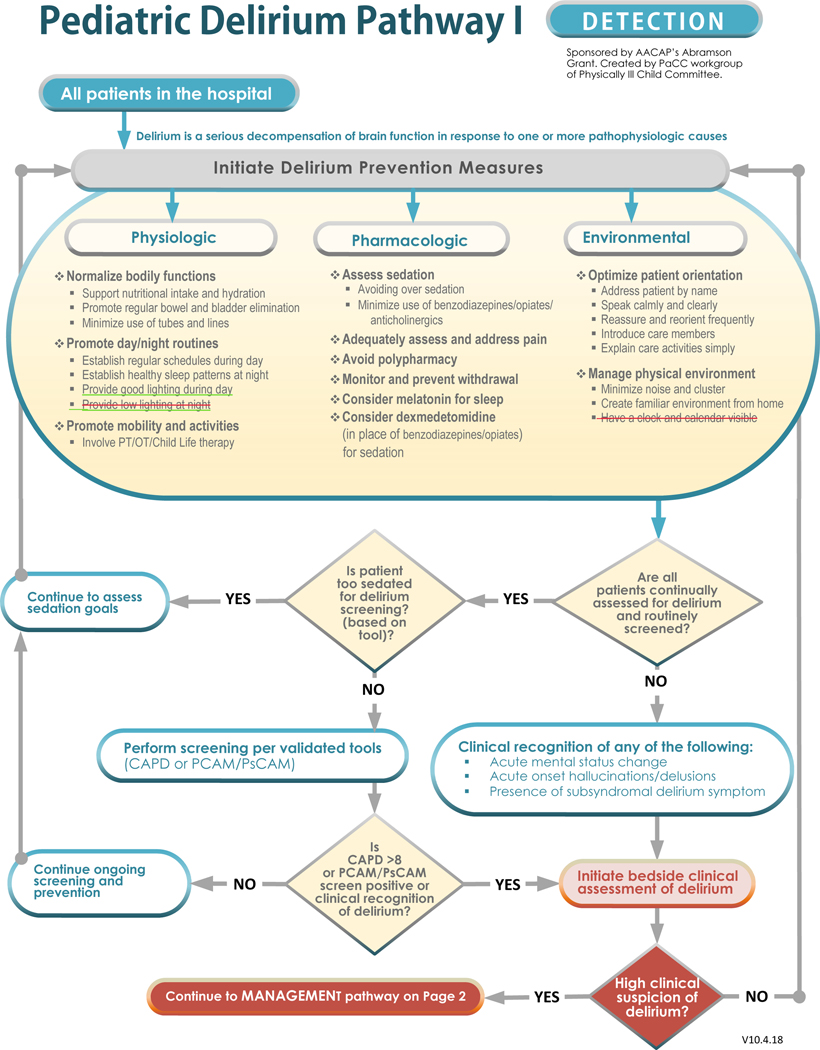
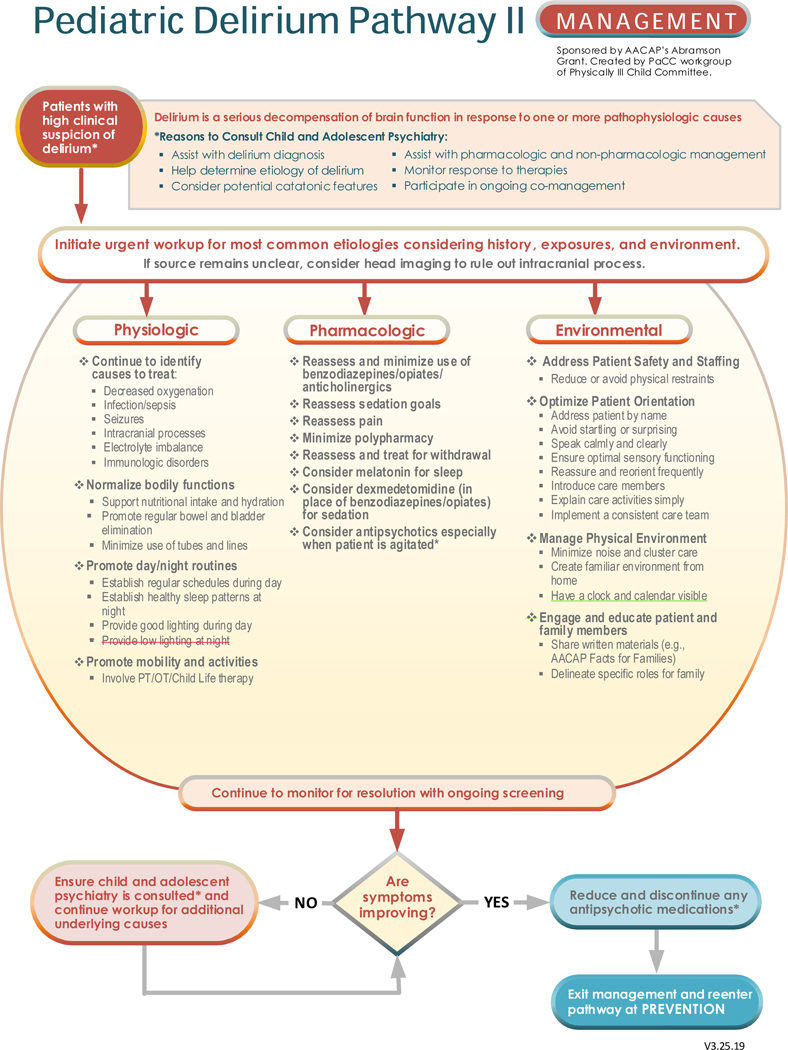
Pediatric delirium is an important comorbidity of medical illness in inpatient pediatric care that has lacked a consistent approach for detection and management. A clinical pathway (CP) was developed to address this need. Pediatric delirium contributes significantly to morbidity, mortality, and costs of inpatient care of medically ill children and adolescents. Screening for delirium in hospital settings with validated tools is feasible and effective in reducing delirium and improving outcomes; however, multidisciplinary coordination is required for implementation. The workgroup, composed of international experts in child and adolescent consultation psychiatry, reviewed the literature and developed a flowchart for feasible screening and management of pediatric delirium. When evidence was lacking, expert consensus was reached; stakeholder feedback was included to create the final pathway. A CP expert collaborated with the workgroup. Two sequential CPs were created: (1) "Prevention and Identification of Pediatric Delirium" emphasizes the need for systematic preventive measures and screening, and (2) "Diagnosis and Management of Pediatric Delirium" recommends an urgent and ongoing search for the underlying causes to reverse the syndrome while providing symptomatic management focused on comfort and safety. Detailed accompanying documents explain the supporting literature and the rationale for recommendations and provide resources such as screening tools and implementation guides. Additionally, the role of the child and adolescent consultation-liaison psychiatrist as a resource for collaborative care of patients with delirium is discussed.
Copyright © 2019 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Similar articles
-
Pediatric Delirium: Evaluation, Management, and Special Considerations.Curr Psychiatry Rep. 2017 Aug 12;19(9):65. doi: 10.1007/s11920-017-0817-3. Curr Psychiatry Rep. 2017. PMID: 28801871 Review.
-
Suicide Risk Screening in Pediatric Hospitals: Clinical Pathways to Address a Global Health Crisis.Psychosomatics. 2019 Jan-Feb;60(1):1-9. doi: 10.1016/j.psym.2018.09.003. Epub 2018 Sep 22. Psychosomatics. 2019. PMID: 30384966 Free PMC article. Review.
-
2022 Society of Critical Care Medicine Clinical Practice Guidelines on Prevention and Management of Pain, Agitation, Neuromuscular Blockade, and Delirium in Critically Ill Pediatric Patients With Consideration of the ICU Environment and Early Mobility.Pediatr Crit Care Med. 2022 Feb 1;23(2):e74-e110. doi: 10.1097/PCC.0000000000002873. Pediatr Crit Care Med. 2022. PMID: 35119438
-
Updates and Clinical Implications of Pediatric Delirium.Crit Care Nurs Clin North Am. 2023 Sep;35(3):315-325. doi: 10.1016/j.cnc.2023.04.006. Epub 2023 Jun 4. Crit Care Nurs Clin North Am. 2023. PMID: 37532385 Review.
-
Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit.Crit Care Med. 2013 Jan;41(1):263-306. doi: 10.1097/CCM.0b013e3182783b72. Crit Care Med. 2013. PMID: 23269131 Review.
Cited by
-
Melatonin Use in Pediatric Intensive Care Units: A Single-Center Experience.Med Sci (Basel). 2023 Aug 28;11(3):55. doi: 10.3390/medsci11030055. Med Sci (Basel). 2023. PMID: 37755159 Free PMC article.
-
Challenges of the Implementation of a Delirium Rate Scale in a Pediatric Intensive Care Unit: A Qualitative Approach.Healthcare (Basel). 2023 Dec 26;12(1):52. doi: 10.3390/healthcare12010052. Healthcare (Basel). 2023. PMID: 38200958 Free PMC article.
-
Risk factors of delirium in paediatric intensive care units: A meta-analysis.PLoS One. 2022 Jul 8;17(7):e0270639. doi: 10.1371/journal.pone.0270639. eCollection 2022. PLoS One. 2022. PMID: 35802701 Free PMC article.
-
Construction of Clinical Pathway Information Management System under the Guidance of Evidence-Based Medicine.J Healthc Eng. 2021 Dec 2;2021:4425449. doi: 10.1155/2021/4425449. eCollection 2021. J Healthc Eng. 2021. Retraction in: J Healthc Eng. 2023 Oct 11;2023:9848029. doi: 10.1155/2023/9848029. PMID: 34900187 Free PMC article. Retracted.
-
Healthcare Providers and Parents Highlight Challenges of Pediatric Hand Fracture Care.Plast Reconstr Surg Glob Open. 2023 Feb 17;11(2):e4815. doi: 10.1097/GOX.0000000000004815. eCollection 2023 Feb. Plast Reconstr Surg Glob Open. 2023. PMID: 36817271 Free PMC article.
References
-
- Schieveld JN, Janssen NJ, van Cauteren YJ. On the Cornell Assessment for Pediatric Delirium and both the diagnostic and statistical manual, 5th edition, and International Classification of Diseases, 11th revision: quo vadis?*. Crit Care Med. 2014;42(3):751–2. - PubMed
-
- American Psychiatric Association. Desk Reference to the Diagnostic Criteria from DSM-5. Washington, DC: American Psychiatric Association. 2013
-
- Maldonado JR. Acute Brain Failure: Pathophysiology, Diagnosis, Management, and Sequelae of Delirium. Crit Care Clin. 2017;33(3):461–519. - PubMed
-
- Cerejeira J, Batista P, Nogueira V, Vaz-Serra A, Mukaetova-Ladinska EB. The stress response to surgery and postoperative delirium: evidence of hypothalamic-pituitary-adrenal axis hyperresponsiveness and decreased suppression of the GH/IGF-1 Axis. J Geriatr Psychiatry Neurol. 2013;26(3):185–94. - PubMed
-
- Cano Londoño EM, Gil IC Mejía, Uribe Hernández K, et al. Delirium during the first evaluation of children aged five to 14 years admitted to a paediatric critical care unit. Intensive Crit Care Nurs. 2018;45:37–43 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
