

Precision medicine in gastric cancer
- PMID: 31662821
- PMCID: PMC6815928
- DOI: 10.4251/wjgo.v11.i10.804
Precision medicine in gastric cancer
Abstract
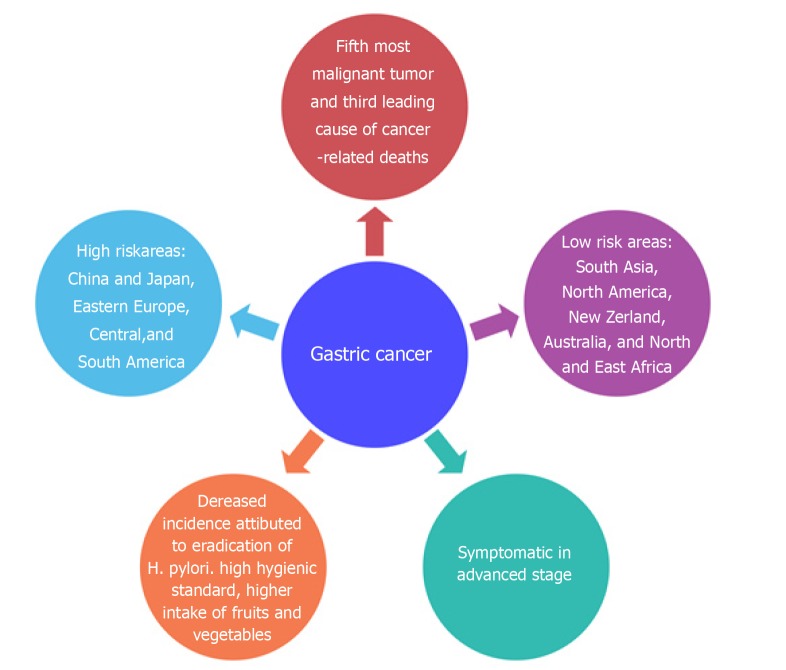
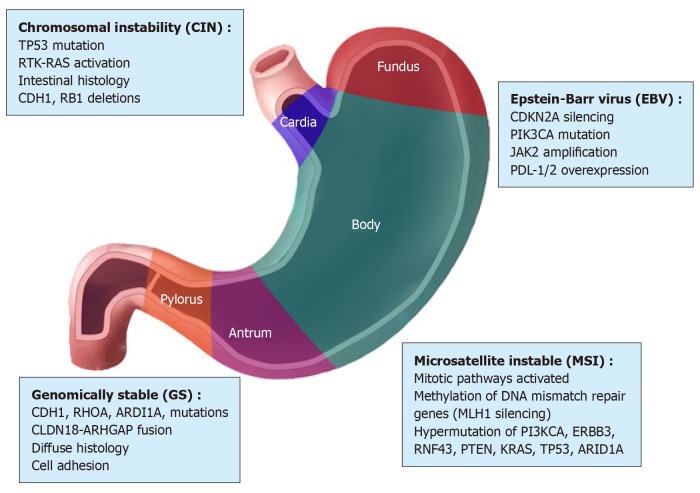
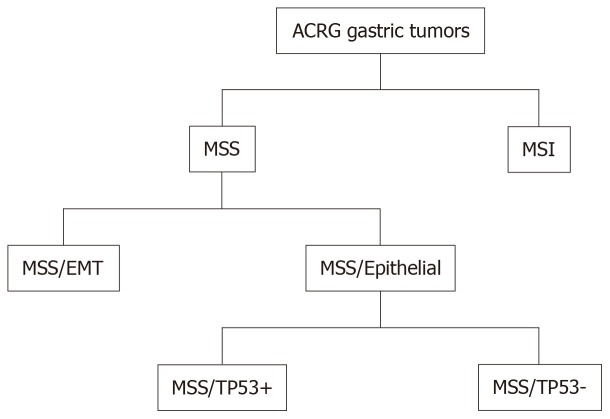
Gastric cancer (GC) is a complex disease linked to a series of environmental factors and unhealthy lifestyle habits, and especially to genetic alterations. GC represents the second leading cause of cancer-related deaths worldwide. Its onset is subtle, and the majority of patients are diagnosed once the cancer is already advanced. In recent years, there have been innovations in the management of advanced GC including the introduction of new classifications based on its molecular characteristics. Thanks to new technologies such as next-generation sequencing and microarray, the Cancer Genome Atlas and Asian Cancer Research Group classifications have also paved the way for precision medicine in GC, making it possible to integrate diagnostic and therapeutic methods. Among the objectives of the subdivision of GC into subtypes is to select patients in whom molecular targeted drugs can achieve the best results; many lines of research have been initiated to this end. After phase III clinical trials, trastuzumab, anti-Erb-B2 receptor tyrosine kinase 2 (commonly known as ERBB2) and ramucirumab, anti-vascular endothelial growth factor receptor 2 (commonly known as VEGFR2) monoclonal antibodies, were approved and introduced into first- and second-line therapies for patients with advanced/metastatic GC. However, the heterogeneity of this neoplasia makes the practical application of such approaches difficult. Unfortunately, scientific progress has not been matched by progress in clinical practice in terms of significant improvements in prognosis. Survival continues to be low in contrast to the reduction in deaths from many common cancers such as colorectal, lung, breast, and prostate cancers. Although several target molecules have been identified on which targeted drugs can act and novel products have been introduced into experimental therapeutic protocols, the overall approach to treating advanced stage GC has not substantially changed. Currently, surgical resection with adjuvant or neoadjuvant radiotherapy and chemotherapy are the most effective treatments for this disease. Future research should not underestimate the heterogeneity of GC when developing diagnostic and therapeutic strategies aimed toward improving patient survival.
Keywords: Biomarkers; Gastric cancer; Molecular characterization; Precision medicine; Targeted therapy.
©The Author(s) 2019. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures
References
-
- Nguyen LT, Uchida T, Murakami K, Fujioka T, Moriyama M. Helicobacter pylori virulence and the diversity of gastric cancer in Asia. J Med Microbiol. 2008;57:1445–1453. - PubMed
-
- Uemura N, Okamoto S, Yamamoto S, Matsumura N, Yamaguchi S, Yamakido M, Taniyama K, Sasaki N, Schlemper RJ. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med. 2001;345:784–789. - PubMed
-
- de Martel C, Forman D, Plummer M. Gastric cancer: epidemiology and risk factors. Gastroenterol Clin North Am. 2013;42:219–240. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
