

Diminished right ventricular function at diagnosis of pulmonary hypertension is associated with mortality in bronchopulmonary dysplasia
- PMID: 31662848
- PMCID: PMC6792284
- DOI: 10.1177/2045894019878598
Diminished right ventricular function at diagnosis of pulmonary hypertension is associated with mortality in bronchopulmonary dysplasia
Abstract
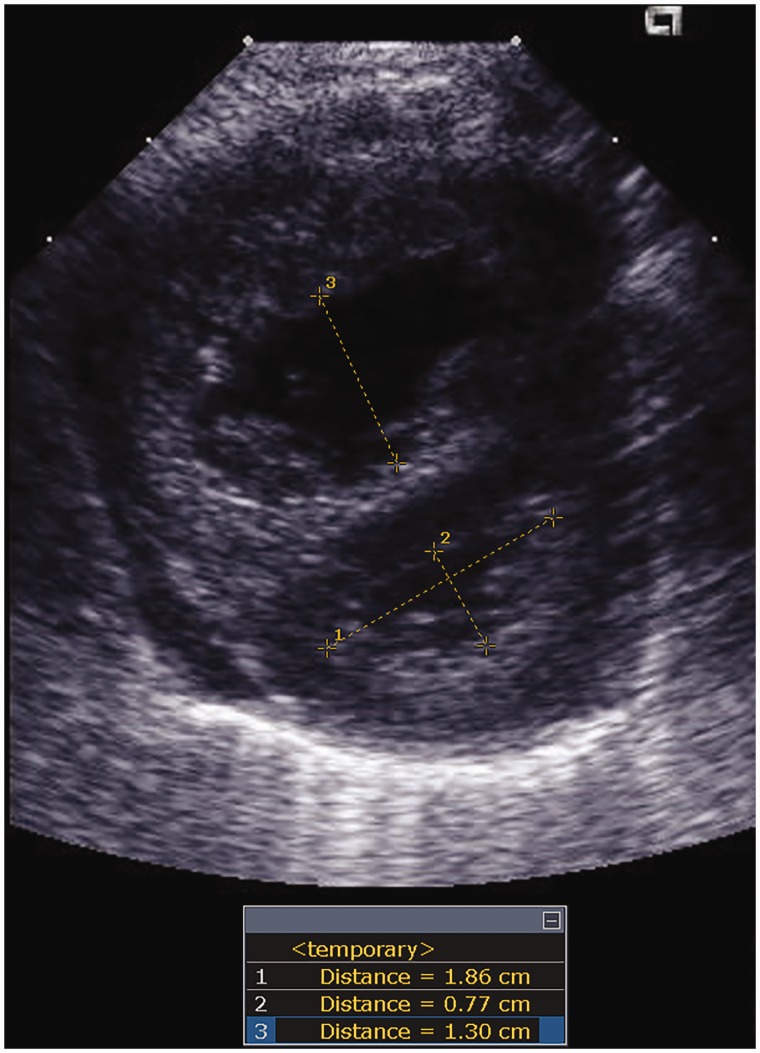
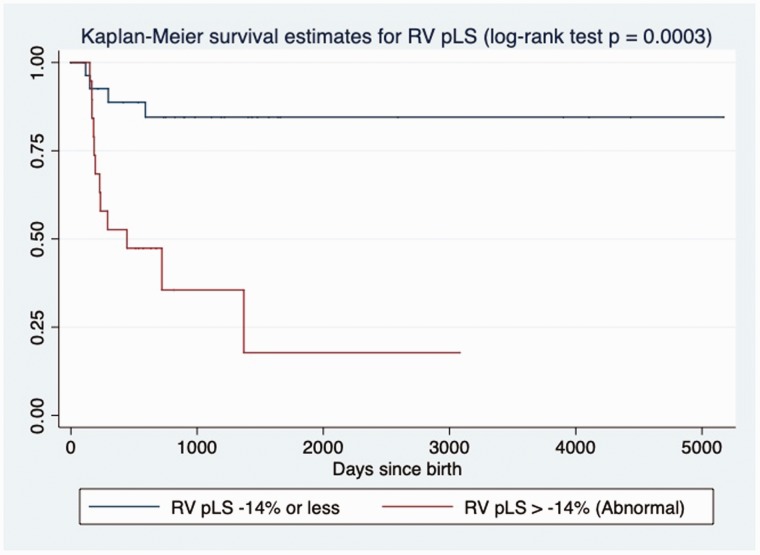
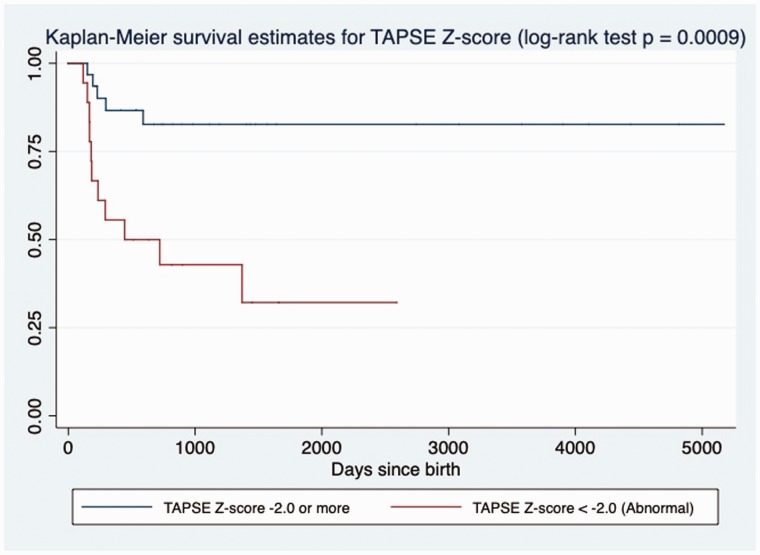
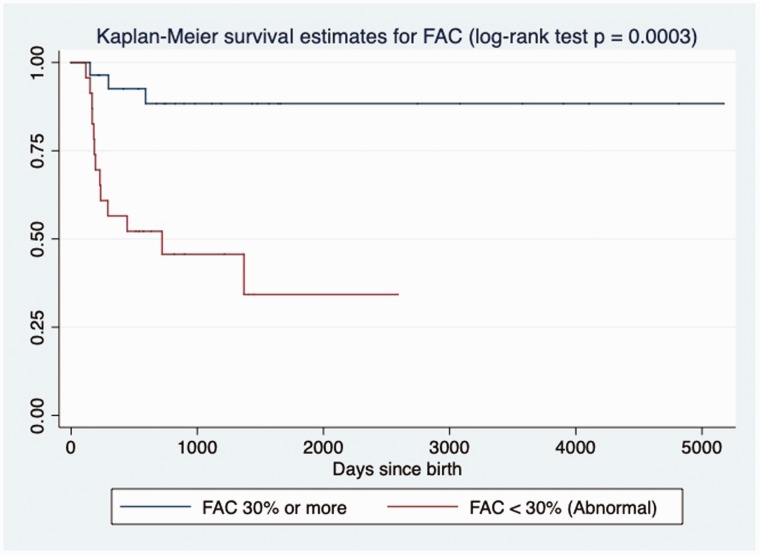
Pulmonary vascular disease and resultant pulmonary hypertension (PH) have been increasingly recognized in the preterm population, particularly among patients with bronchopulmonary dysplasia (BPD). Limited data exist on the impact of PH severity and right ventricular (RV) dysfunction at PH diagnosis on outcome. The purpose of this study was to evaluate if echocardiography measures of cardiac dysfunction and PH severity in BPD-PH were associated with mortality. The study is a retrospective analysis of the echocardiography at three months or less from time of PH diagnosis. Survival analysis using a univariate Cox proportional hazard model is presented and expressed using hazard ratios (HR). We included 52 patients with BPD and PH of which 16 (31%) died at follow-up. Average gestational age at birth was 26.3 ± 2.3 weeks. Echocardiography was performed at a median of 43.3 weeks (IQR: 39.0-54.7). The median time between PH diagnosis and death was 117 days (range: 49-262 days). Multiple measures of PH severity and RV performance were associated with mortality (sPAP/sBP: HR 1.02, eccentricity index: HR 2.02, tricuspid annular plane systolic excursion Z-score: HR 0.65, fractional area change: HR 0.88, peak longitudinal strain: HR 1.22). Hence, PH severity and underlying RV dysfunction at PH diagnosis were associated with mortality in BPD-PH patients. While absolute estimation of pulmonary pressures is not feasible in every screening echocardiography, thorough evaluation of RV function and other markers of PH may allow to discriminate the most at-risk population and should be considered as standard add-ons to the current screening at 36 weeks.
Keywords: bronchopulmonary dysplasia; prematurity; pulmonary hypertension; speckle-tracking echocardiography; strain.
© The Author(s) 2019.
Figures
References
-
- Abman SH, Hansmann G, Archer SL, et al. Pediatric pulmonary hypertension: guidelines from the american heart association and american thoracic society. Cir 2015; 132: 2037–2099. - PubMed
LinkOut - more resources
Full Text Sources
