

Acute Kidney Injury in Critically Ill Children and Subsequent Chronic Kidney Disease
- PMID: 31662875
- PMCID: PMC6794652
- DOI: 10.1177/2054358119880188
Acute Kidney Injury in Critically Ill Children and Subsequent Chronic Kidney Disease
Abstract
Background: The progression from acute kidney injury (AKI) to chronic kidney disease (CKD) is not well understood in children.
Objectives: We aimed to develop a pediatric CKD definition using administrative data and use it to evaluate the association between AKI in critically ill children and CKD 5 years after hospital discharge.
Design: Retrospective cohort study using chart collection and administrative data.
Setting: Two-center study in Montreal, Canada.
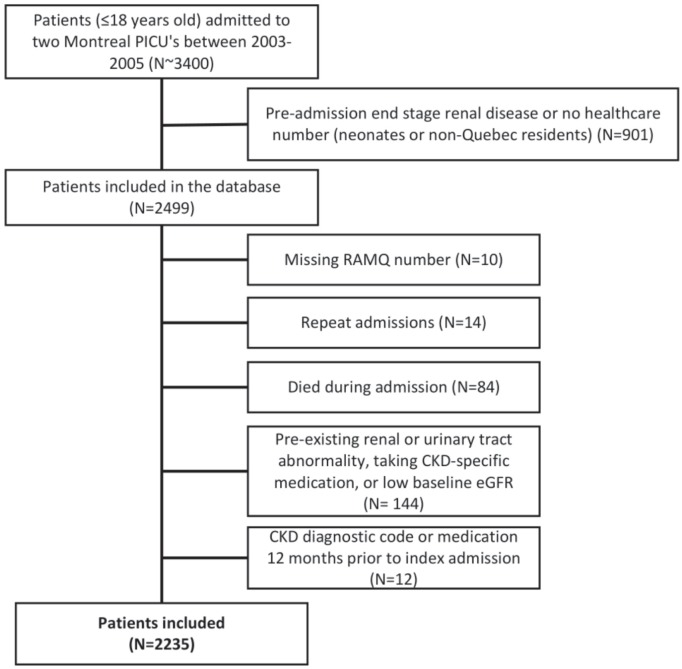
Patients: Children (≤18 years old) admitted to two pediatric intensive care units (ICUs) between 2003 and 2005. We a priori excluded patients with end-stage renal disease or no health care number. Only the first admission during the study period was included. We excluded patients who could not be linked to administrative data, did not survive hospitalization, or had preexisting renal disease.
Measurements: Acute kidney injury was defined using Kidney Disease: Improving Global Outcomes (KDIGO) criteria. Patients were defined as having CKD 5 years post-discharge if they had ≥1 CKD diagnostic code or ≥1 CKD-specific medication prescription.
Methods: Chart data used to define the exposure (AKI) were merged with provincial administrative data used to define the outcome (CKD). Cox regression was used to evaluate the AKI-CKD association.
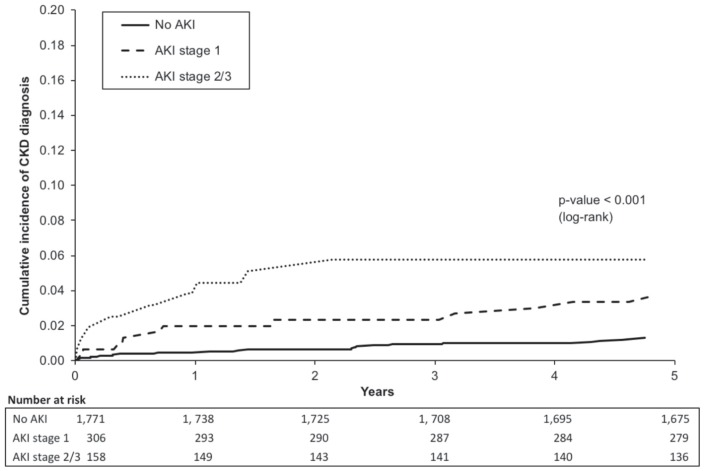
Results: A total of 2235 (56% male) patients were included, and the median admission age was 3.7 years. A total of 464 (21%) patients developed AKI during pediatric ICU admission. At 5 years post-discharge, 43 (2%) patients had a CKD diagnosis. Patients with both stage 1 and stage 2-3 AKI had increased risk of a CKD diagnosis, with the adjusted hazard ratios (95% confidence intervals) of 2.2 (1.1-4.5) and 2.5 (1.1-5.7), respectively (P < .001).
Limitations: Results may not be generalizable to non-ICU patients. We were not able to control for post-discharge variables; future research should try to explore these additional potential risk factors further.
Conclusions: Acute kidney injury is associated with 5-year post-discharge CKD diagnosis defined by administrative health care data.
Contexte: Chez l’enfant, la progression de l’insuffisance rénale aigüe (IRA) vers l’insuffisance rénale chronique (IRC) est encore mal connue.
Objectifs: Nous souhaitions élaborer une définition de l’IRC pédiatrique à partir des données administratives, et l’employer pour évaluer l’association entre l’IRA chez les enfants gravement malades et un diagnostic d’IRC cinq ans après leur sortie de l’hôpital.
Type d’étude: Étude de cohorte rétrospective réalisée à partir des dossiers médicaux et des données administratives.
Cadre: Deux centres hospitaliers de Montréal (Canada).
Sujets: L’étude porte sur des enfants (≤18 ans) admis à deux unités de soins intensifs (USI) pédiatriques entre 2003 et 2005. Les patients atteints d’insuffisance rénale terminale ou sans numéro d’assurance-maladie ont été exclus d’emblée. Seule la première admission survenue au cours de l’étude a été retenue. Les patients n’ayant pu être reliés aux données administratives, n’ayant pas survécu à l’hospitalisation ou souffrant d’une néphropathie préexistante ont été exclus.
Mesures: L’IRA a été définie selon les critères KDIGO (Kidney Disease: Improving Global Outcomes) et l’IRC cinq ans après la sortie de l’hôpital par la présence d’au moins un code diagnostique pour l’IRC ou la prise d’au moins un médicament spécifique au traitement de l’IRC.
Méthodologie: Les données des dossiers médicaux, utilisées pour définir l’exposition (IRA), ont été couplées aux données administratives provinciales, utilisées pour définir le résultat (IRC). Un modèle de régression de Cox a servi à établir l’association entre IRA et IRC.
Résultats: Ont été inclus 2 235 patients (56 % de garçons), dont l’âge médian à l’admission était de 3,7 ans. De ce nombre, 464 (21 %) ont développé une IRA en cours d’hospitalisation à l’USI pédiatrique. Cinq ans après leur sortie de l’hôpital, 43 patients (2 %) avaient reçu un diagnostic d’IRC. Les patients atteints d’une IRA de stade 1 et de stade 2-3 ont présenté un plus grand risque de progresser vers l’IRC (rapport de risque ajusté [IC à 95 %] 2,2 [1,1 – 4,5] et 2,5 [1,1 – 5,7] respectivement, P < 0,001).
Limites: Les résultats pourraient ne pas s’appliquer aux patients non admis aux USI pédiatriques. Nous n’avons pu ajuster les résultats avec les variables après la sortie de l’hôpital. Des études futures devraient examiner plus attentivement ces potentiels facteurs de risque supplémentaires.
Conclusion: L’IRA chez l’enfant a été associée à une progression vers l’IRC cinq ans après la sortie de l’hôpital, telle que définie par les données administratives de santé.
Keywords: acute kidney injury; administrative data; children; chronic kidney disease; pediatrics.
© The Author(s) 2019.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Alkandari O, Eddington KA, Hyder A, et al. Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: a two-center retrospective cohort study. Crit Care. 2011;15(3):R146. doi:10.1186/cc10269. - DOI - PMC - PubMed
-
- Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int. 2012;81(5):442-448. http://www.nature.com/ki/journal/v81/n5/suppinfo/ki2011379s1.html. Accessed August 19, 2015. - PMC - PubMed
LinkOut - more resources
Full Text Sources
