

Chlorogenic Acid Attenuates Kidney Ischemic/Reperfusion Injury via Reducing Inflammation, Tubular Injury, and Myofibroblast Formation
- PMID: 31662982
- PMCID: PMC6778937
- DOI: 10.1155/2019/5423703
Chlorogenic Acid Attenuates Kidney Ischemic/Reperfusion Injury via Reducing Inflammation, Tubular Injury, and Myofibroblast Formation
Abstract
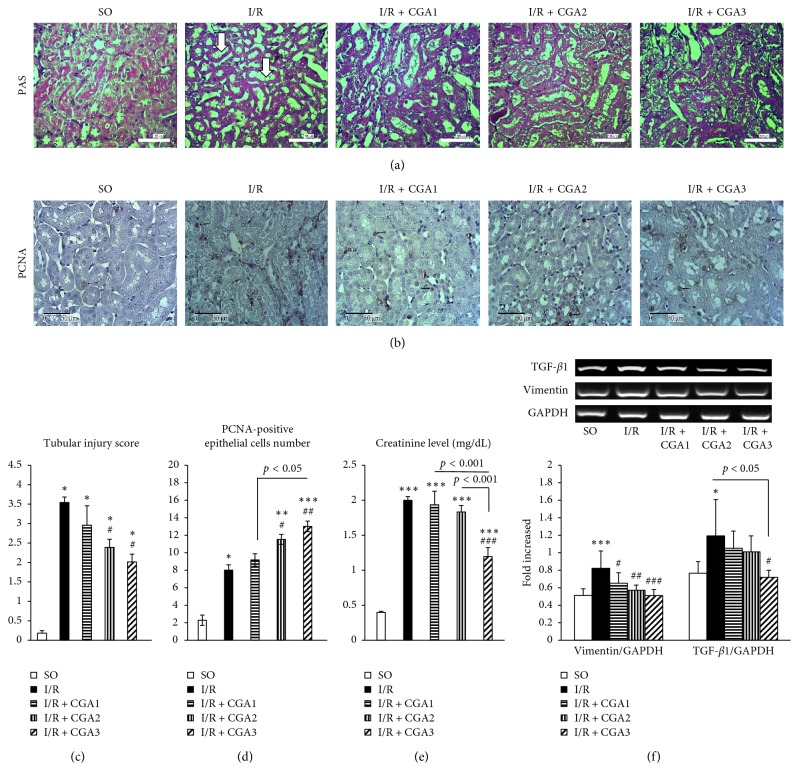
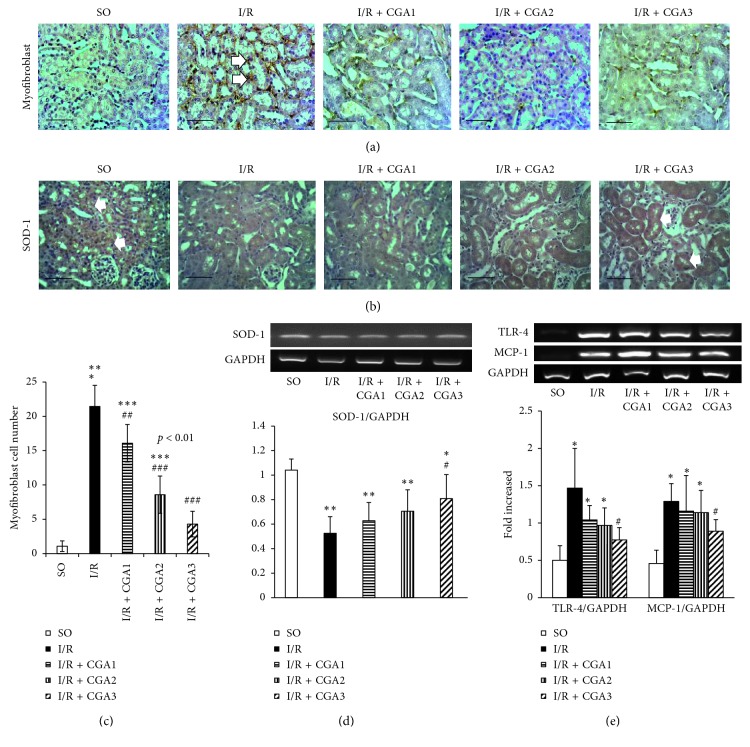
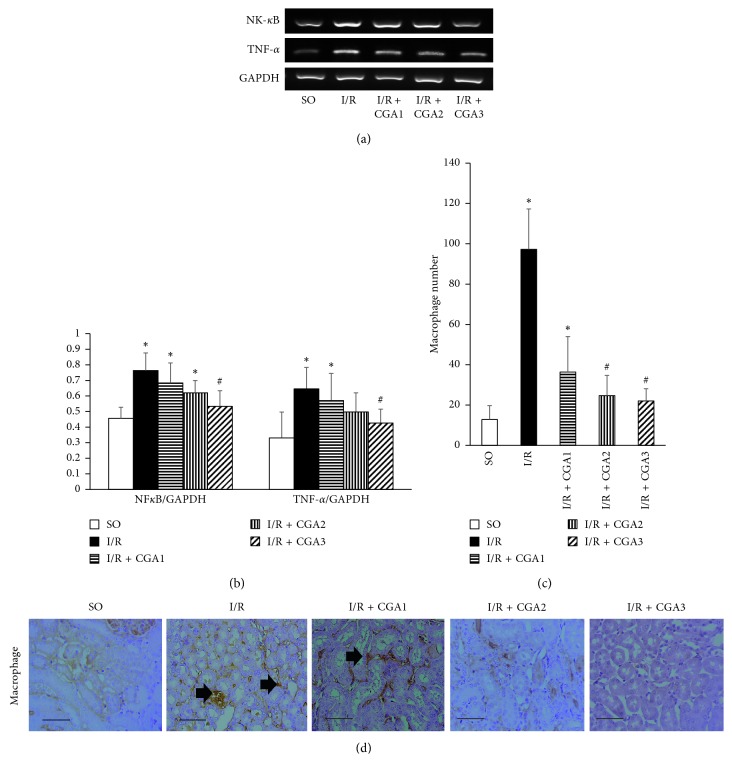
Kidney ischemic/reperfusion (I/R) injury is the main cause of acute kidney injury (AKI) involving renal function deterioration, renal architecture damage, and inflammation. This condition may lead to kidney fibrosis with epithelial to mesenchymal transition (EMT) and myofibroblast formation. Inhibition of chronic effects of kidney I/R injury may provide effective strategies for treating AKI and chronic kidney diseases (CKDs). Chlorogenic acid (CGA) is recognized as a powerful antioxidant, with anti-inflammatory and antifibrotic properties in many conditions. However, the effect of CGA on kidney I/R injury has not been elucidated yet. Kidney I/R injury was performed on male Swiss background mice (I/R group, n = 5, 3-4 months, 30-40 g) which underwent bilateral renal pedicles clamping for 30 minutes and then were euthanized on day three after operation. Three groups of I/R were treated with 3 different doses of CGA intraperitoneally for 2 days: 3.5 (I/R + CGA1 group), 7 (I/R + CGA2 group), and 14 (I/R + CGA3 group) mg/kg of body weight. Tubular injury was quantified based on Periodic Acid-Schiff staining, while reverse transcriptase PCR (RT-PCR) was performed to quantify mRNA expression of TGF-β1, vimentin, SOD-1, TLR-4, TNF-α, NF-κB and MCP-1. Immunohistochemical staining was done to quantify proliferating cell nuclear antigen (PCNA), myofibroblast (α-SMA), SOD-1 and macrophage (CD68) number. Kidney I/R demonstrated tubular injury and increased inflammatory mediator expression, macrophage number, and myofibroblast expansion. Meanwhile, histological analysis showed lower tubular injury with higher epithelial cell proliferation in CGA-treated groups compared to the I/R group. RT-PCR also revealed significantly lower TGF-β1 and vimentin mRNA expressions with higher SOD-1 mRNA expression. CGA-treated groups also demonstrated a significantly lower macrophage and myofibroblast number compared to the I/R group. These findings associated with lower mRNA expression of TLR-4, TNF-α, NF-κB, and MCP-1 as inflammatory mediators in CGA groups. I/R + CGA3 represented the highest amelioration effect among other CGA-treated groups. CGA treatment attenuates kidney I/R injury through reducing inflammation, decreasing myofibroblast expansion, and inducing epithelial cells proliferation.
Copyright © 2019 Nur Arfian et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
