

Development and Validation of a Nomogram for Early Detection of Malignant Gallbladder Lesions
- PMID: 31663905
- PMCID: PMC6884352
- DOI: 10.14309/ctg.0000000000000098
Development and Validation of a Nomogram for Early Detection of Malignant Gallbladder Lesions
Abstract
Objectives: Preoperative decision-making for differentiating malignant from benign lesions in the gallbladder remains challenging. We aimed to create a diagnostic nomogram to identify gallbladder cancer (GBC), especially for incidental GBC (IGBC), before surgical resection.
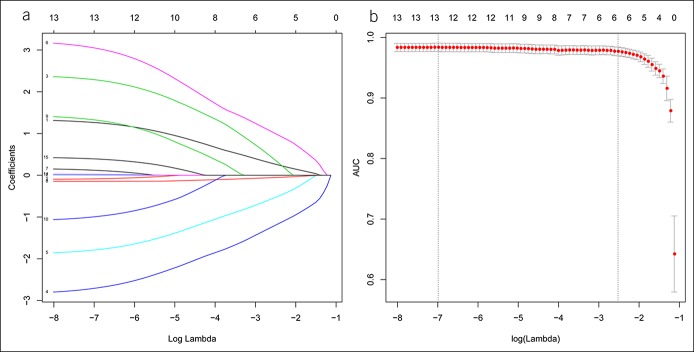
Methods: A total of 587 consecutive patients with pathologically confirmed gallbladder lesions from a hospital were randomly assigned to a training cohort (70%) and an internal validation cohort (30%), with 287 patients from other centers as an external validation cohort. Radiological features were developed by the least absolute shrinkage and selection operator logistic regression model. Significant radiological features and independent clinical factors, identified by multivariate analyses, were used to construct a nomogram.
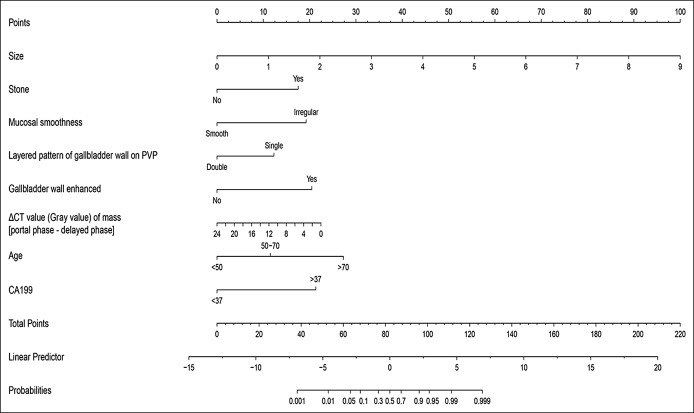
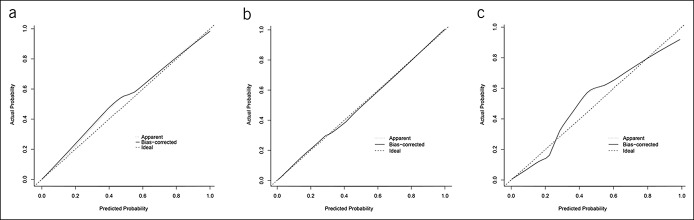
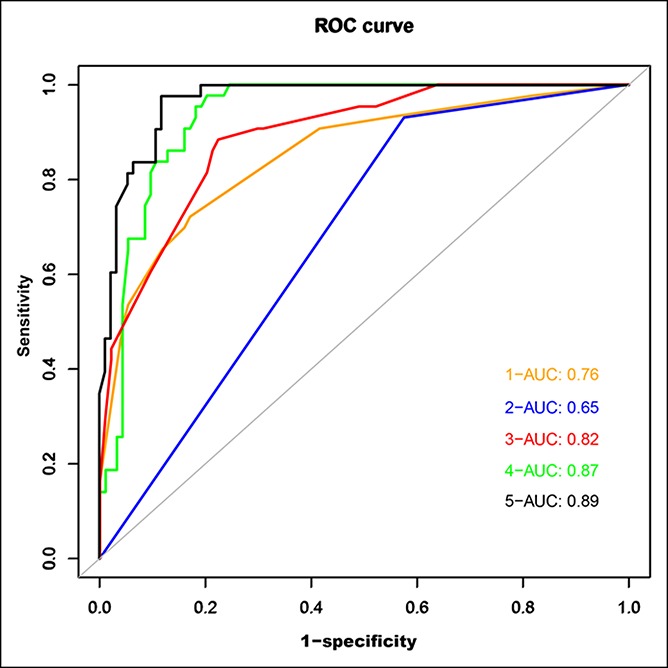
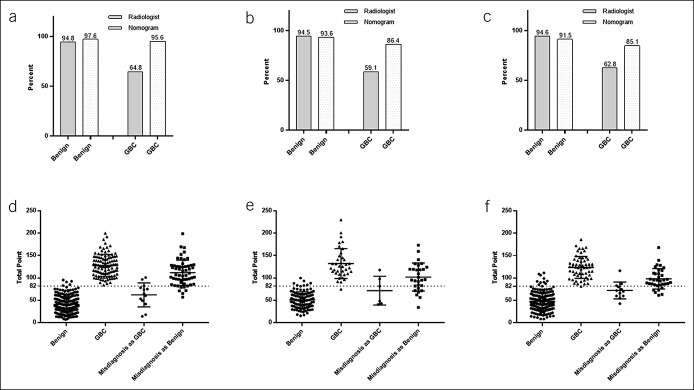
Results: A diagnostic nomogram was established by age, CA19.9, and 6 radiological features. The values of area under the curve in the internal and external validation cohorts were up to 0.91 and 0.89, respectively. The calibration curves for probability of GBC showed optimal agreement between nomogram prediction and actual observation. Compared with previous methods, it demonstrated superior sensitivity (91.5%) and accuracy (85.1%) in the diagnosis of GBC. The accuracy using the nomogram was significantly higher in GBC groups compared with that by radiologists in the training cohort (P < 0.001) and similarly in each cohort. Notably, most of the IGBC, which were misdiagnosed as benign lesions, were successfully identified using this nomogram.
Discussion: A novel nomogram provides a powerful tool for detecting the presence of cancer in gallbladder masses, with an increase in accuracy and sensitivity. It demonstrates an unprecedented potential for IGBC identification.
Figures
References
-
- Myers RP, Shaffer EA, Beck PL. Gallbladder polyps: Epidemiology, natural history and management. Can J Gastroenterol 2002;16:187–94. - PubMed
-
- Hardy MA, Volk H. Primary carcinoma of the gallbladder. A ten year review. Am J Surg 1970;120:800–3. - PubMed
-
- Ferretti S, Gafa L. Upper gastrointestinal tract cancers: Oesophagus, stomach, liver, gallbladder and biliary ducts, pancreas. Epidemiol Prev 2004;28:34–42. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
