

Monotherapy versus combination therapy for multidrug-resistant Gram-negative infections: Systematic Review and Meta-Analysis
- PMID: 31664064
- PMCID: PMC6821042
- DOI: 10.1038/s41598-019-51711-x
Monotherapy versus combination therapy for multidrug-resistant Gram-negative infections: Systematic Review and Meta-Analysis
Abstract
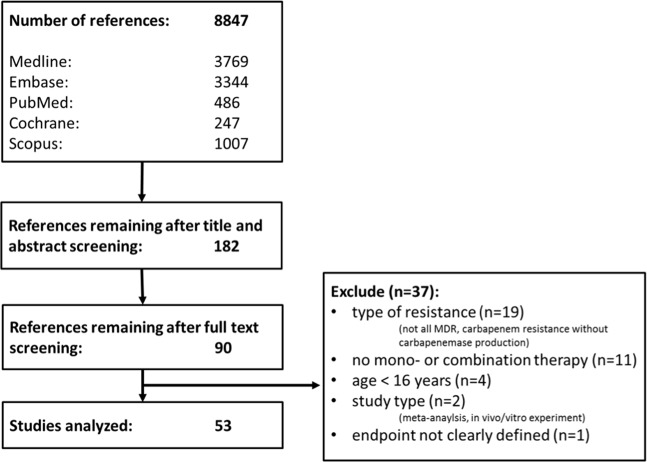
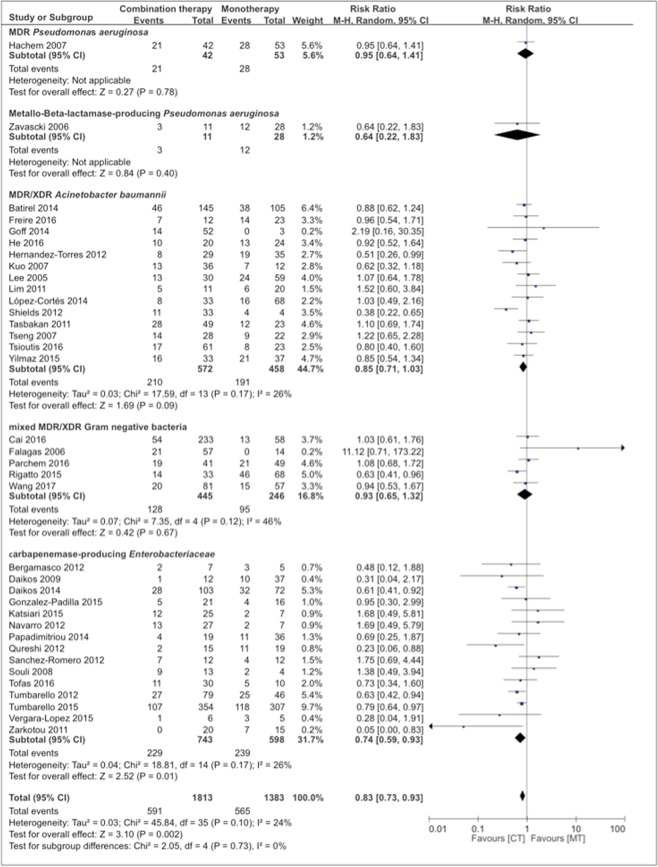
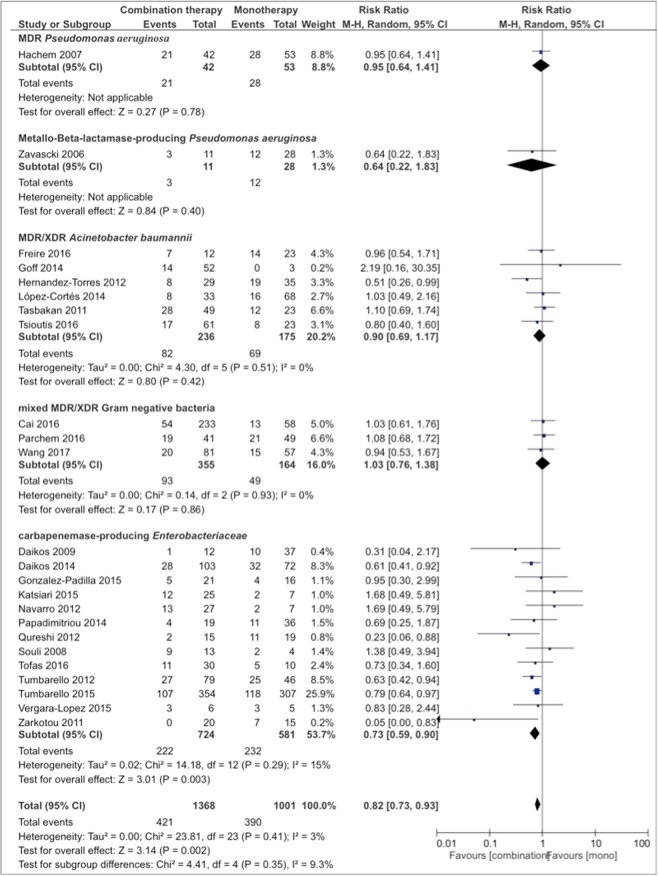
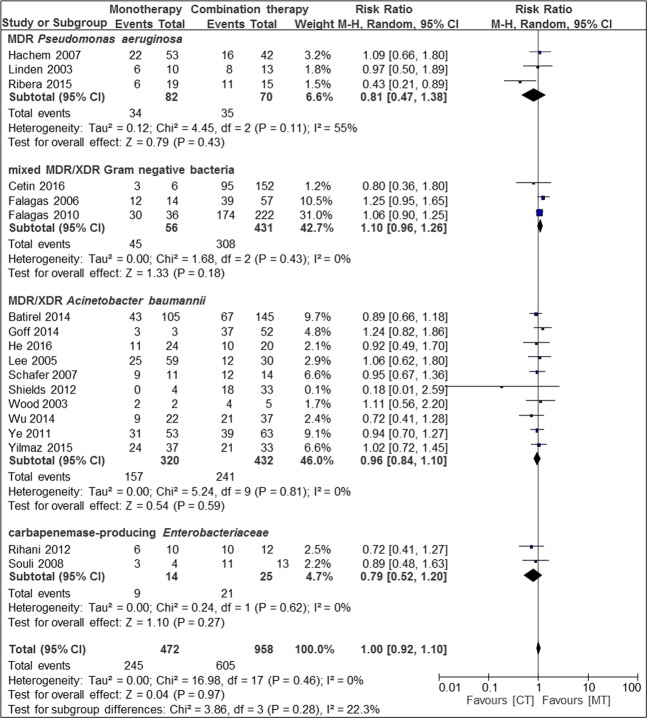
Infections caused by carbapenemase-producing, multidrug-resistant (MDR), or extensively drug-resistant (XDR) Gram-negative bacteria constitute a major therapeutic challenge. Whether combination antibiotic therapy is superior to monotherapy remains unknown. In this systematic review and meta-analysis OVID MEDLINE, EMBASE, PubMed, The Cochrane Library, and Scopus databases were searched for randomized controlled trials (RCTs) and observational studies published by December 2016 comparing mono- with combination antibiotic therapy for infections with carbapenemase-producing, MDR, or XDR Gram-negative bacteria. Mortality and clinical cure rates served as primary and secondary outcome measures, respectively. Of 8847 initially identified studies, 53 studies - covering pneumonia (n = 10 studies), blood stream (n = 15), osteoarticular (n = 1), and mixed infections (n = 27) - were included. 41% (n = 1848) of patients underwent monotherapy, and 59% (n = 2666) combination therapy. In case series/cohort studies (n = 45) mortality was lower with combination- vs. monotherapy (RR 0.83, CI 0.73-0.93, p = 0.002, I2 = 24%). Subgroup analysis revealed lower mortality with combination therapy with at least two in-vitro active antibiotics, in blood stream infections, and carbapenemase-producing Enterobacteriaceae. No mortality difference was seen in case-control studies (n = 6) and RCTs (n = 2). Cure rates did not differ regardless of study type. The two included RCTs had a high and unknown risk of bias, respectively. 16.7% (1/6) of case-control studies and 37.8% (17/45) of cases series/cohort studies were of good quality, whereas quality was poor in the remaining studies. In conclusion, combination antimicrobial therapy of multidrug-resistant Gram-negative bacteria appears to be superior to monotherapy with regard to mortality.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Cochrane Collaboration Cochrane Handbook for Systematic Reviews of Interventions, http://handbook.cochrane.org/ - PubMed
-
- Wells, G. E. A. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available at, http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. (2011).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
