

A prospective international multi-center study on safety and efficacy of deep brain stimulation for resistant obsessive-compulsive disorder
- PMID: 31664175
- PMCID: PMC7985042
- DOI: 10.1038/s41380-019-0562-6
A prospective international multi-center study on safety and efficacy of deep brain stimulation for resistant obsessive-compulsive disorder
Abstract
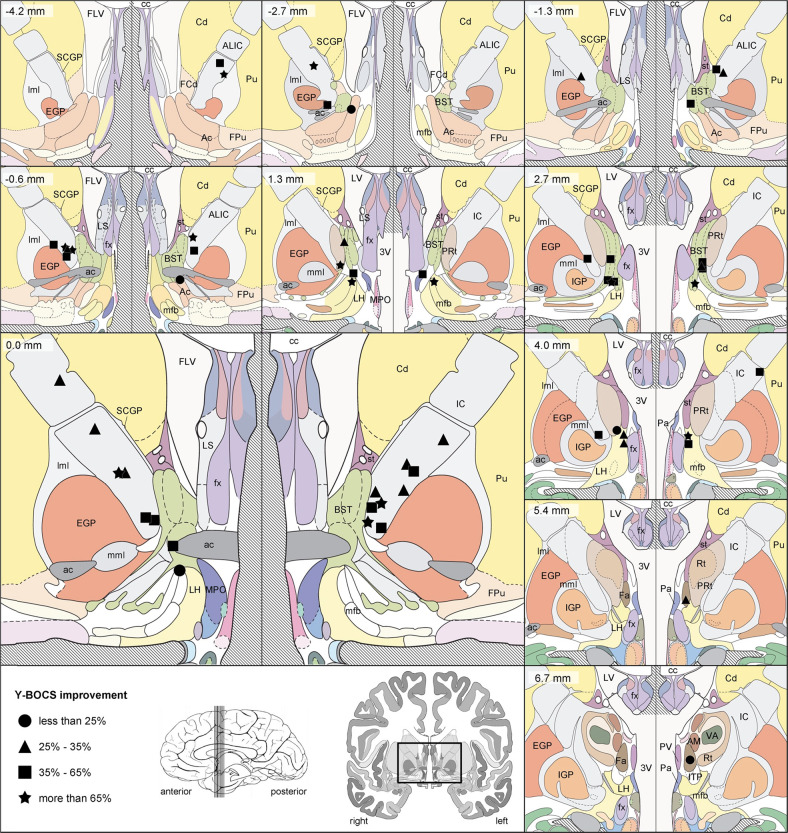
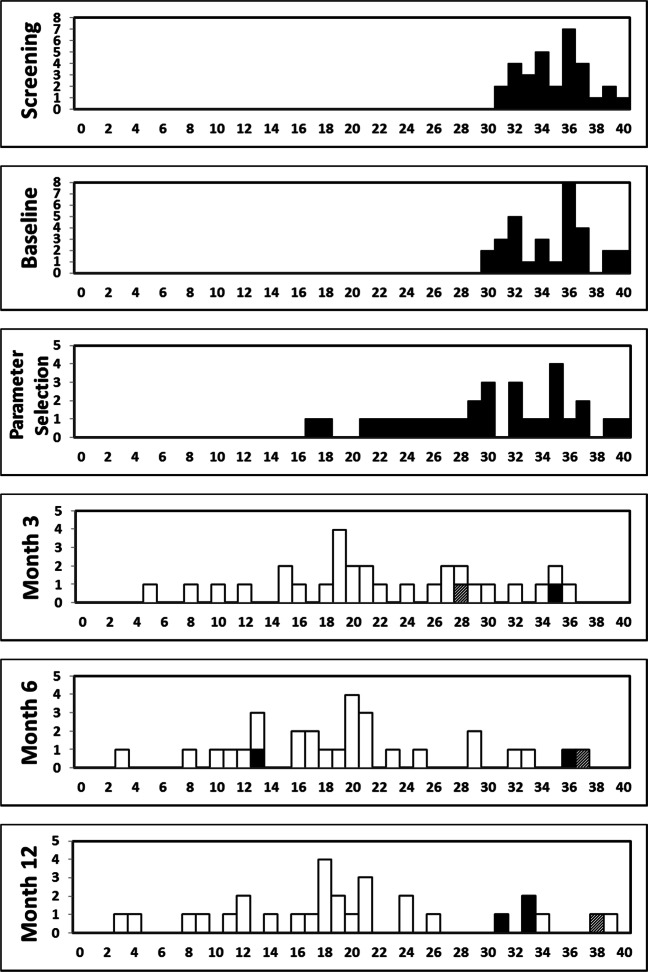
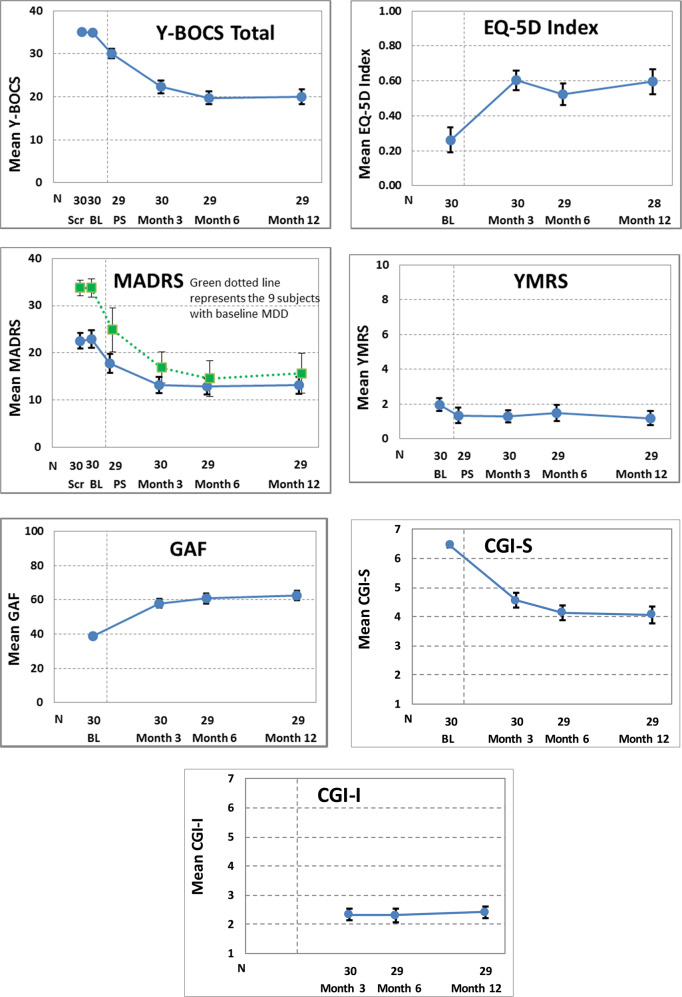
Deep brain stimulation (DBS) has been proposed for severe, chronic, treatment-refractory obsessive-compulsive disorder (OCD) patients. Although serious adverse events can occur, only a few studies report on the safety profile of DBS for psychiatric disorders. In a prospective, open-label, interventional multi-center study, we examined the safety and efficacy of electrical stimulation in 30 patients with DBS electrodes bilaterally implanted in the anterior limb of the internal capsule. Safety, efficacy, and functionality assessments were performed at 3, 6, and 12 months post implant. An independent Clinical Events Committee classified and coded all adverse events (AEs) according to EN ISO14155:2011. All patients experienced AEs (195 in total), with the majority of these being mild (52% of all AEs) or moderate (37%). Median time to resolution was 22 days for all AEs and the etiology with the highest AE incidence was 'programming/stimulation' (in 26 patients), followed by 'New illness, injury, condition' (13 patients) and 'pre-existing condition, worsening or exacerbation' (11 patients). Sixteen patients reported a total of 36 serious AEs (eight of them in one single patient), mainly transient anxiety and affective symptoms worsening (20 SAEs). Regarding efficacy measures, Y-BOCS reduction was 42% at 12 months and the responder rate was 60%. Improvements in GAF, CGI, and EuroQol-5D index scores were also observed. In sum, although some severe AEs occurred, most AEs were mild or moderate, transient and related to programming/stimulation and tended to resolve by adjustment of stimulation. In a severely treatment-resistant population, this open-label study supports that the potential benefits outweigh the potential risks of DBS.
Conflict of interest statement
TCB, FG, and TB are employees of Medtronic and received standard salaries during the conduct of the study. LB received personal fees for study design and data collection during the conduct of the study. BN is the first author on a patent on DBS for OCD, and received grants as Chair ‘Neuromodulation, an endowment from Medtronic’ and ‘Neurosurgery for Psychiatric Disorders’, from Medtronic during the conduct of the study. AK, MP and BZ received grants from Medtronic during the conduct of the study. RE received compensation and equipment support, MS received funding of study procedures and VT received funding of travelcosts, all them from Medtronic during the conduct of the study. Bellvitge University Hospital and Fondazione IRCCS Istituto Naz Neurologico C.Besta received partial financial support for the conduct of the study.
Figures
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, Fifth ed. Washington, DC, USA: American Psychiatric Association; 2013.
-
- The global burden of disease: 2004 update. World Health Organization, WHO Press, Switzerland. ISBN 978 92 4 156371 0. (https://www.who.int/healthinfo/global_burden_disease/GBD_report_2004upda...).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
