Epidemiology of intra-abdominal infection and sepsis in critically ill patients: "AbSeS", a multinational observational cohort study and ESICM Trials Group Project
- PMID: 31664501
- PMCID: PMC6863788
- DOI: 10.1007/s00134-019-05819-3
Epidemiology of intra-abdominal infection and sepsis in critically ill patients: "AbSeS", a multinational observational cohort study and ESICM Trials Group Project
Abstract
Purpose: To describe the epidemiology of intra-abdominal infection in an international cohort of ICU patients according to a new system that classifies cases according to setting of infection acquisition (community-acquired, early onset hospital-acquired, and late-onset hospital-acquired), anatomical disruption (absent or present with localized or diffuse peritonitis), and severity of disease expression (infection, sepsis, and septic shock).
Methods: We performed a multicenter (n = 309), observational, epidemiological study including adult ICU patients diagnosed with intra-abdominal infection. Risk factors for mortality were assessed by logistic regression analysis.
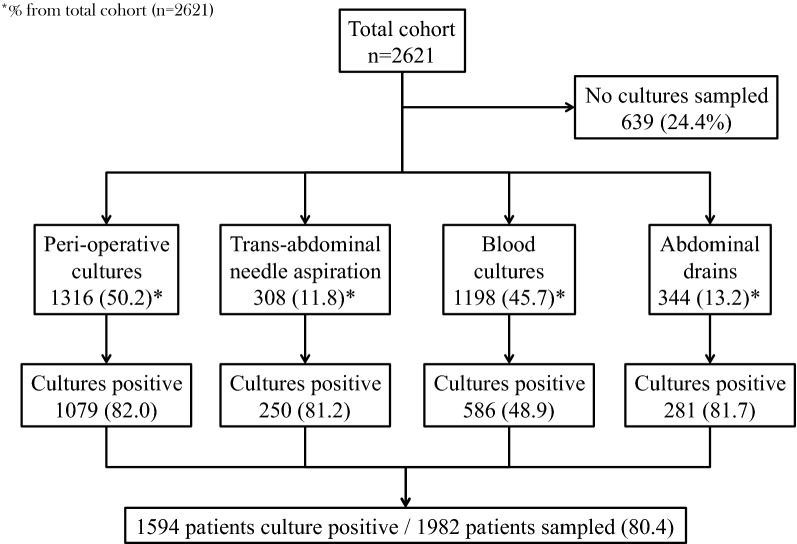
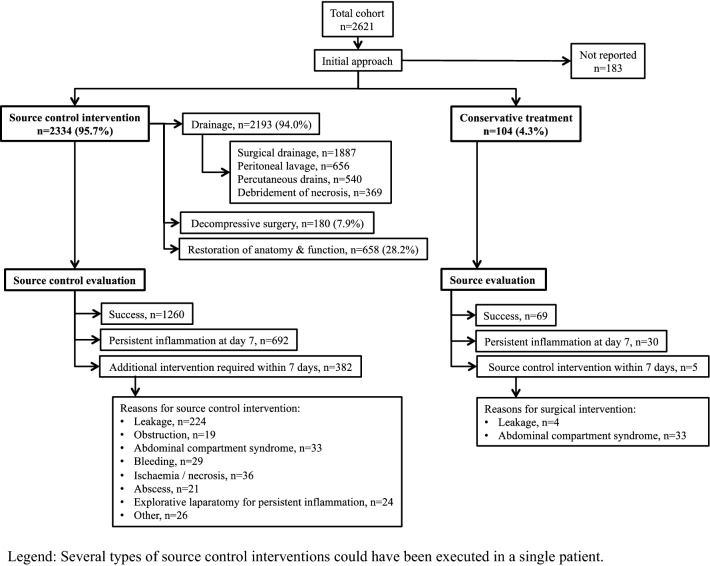
Results: The cohort included 2621 patients. Setting of infection acquisition was community-acquired in 31.6%, early onset hospital-acquired in 25%, and late-onset hospital-acquired in 43.4% of patients. Overall prevalence of antimicrobial resistance was 26.3% and difficult-to-treat resistant Gram-negative bacteria 4.3%, with great variation according to geographic region. No difference in prevalence of antimicrobial resistance was observed according to setting of infection acquisition. Overall mortality was 29.1%. Independent risk factors for mortality included late-onset hospital-acquired infection, diffuse peritonitis, sepsis, septic shock, older age, malnutrition, liver failure, congestive heart failure, antimicrobial resistance (either methicillin-resistant Staphylococcus aureus, vancomycin-resistant enterococci, extended-spectrum beta-lactamase-producing Gram-negative bacteria, or carbapenem-resistant Gram-negative bacteria) and source control failure evidenced by either the need for surgical revision or persistent inflammation.
Conclusion: This multinational, heterogeneous cohort of ICU patients with intra-abdominal infection revealed that setting of infection acquisition, anatomical disruption, and severity of disease expression are disease-specific phenotypic characteristics associated with outcome, irrespective of the type of infection. Antimicrobial resistance is equally common in community-acquired as in hospital-acquired infection.
Keywords: Intensive care; Intra-abdominal infection; Mortality; Multidrug resistance; Peritonitis; Sepsis.
Conflict of interest statement
Received grants related to the submitted work: S. Blot (Pfizer). Received honoraria or grants outside the submitted work: M. Antonelli (Fresenius, Pfizer, Toray); J. De Waele (Research Foundation Flanders, Pfizer, Bayer, MSD); C. Eckmann (Merck, Pfizer); J. Lipman (MSD, Pfizer); E. Maseda (Astellas Pharma, Pfizer, MSD); All other authors: no conflict of interest.
Figures