

Resection of intrahepatic cholangiocarcinoma in elderly patients - is it reasonable?
- PMID: 31664988
- PMCID: PMC6819605
- DOI: 10.1186/s12893-019-0620-7
Resection of intrahepatic cholangiocarcinoma in elderly patients - is it reasonable?
Abstract
Background: Intrahepatic cholangiocarinoma (ICC) has a rising incidence in western countries. Often major or extended resections are necessary for complete tumor removal. Due to demographical trends the number of elderly patients diagnosed with ICC is rising accordingly. Aim of this study is to show whether resection of ICC in elderly patients is reasonable or not.
Methods: Between January 2008 and June 2018 all consecutive patients with ICC were collected. Analyses were focussed on the performed resection, its extent, postoperative morbidity and mortality as well as survival. Statistics were performed with Chi2 test for categorical data and for survival analyses the Kaplan Meier model with log rank test was used.
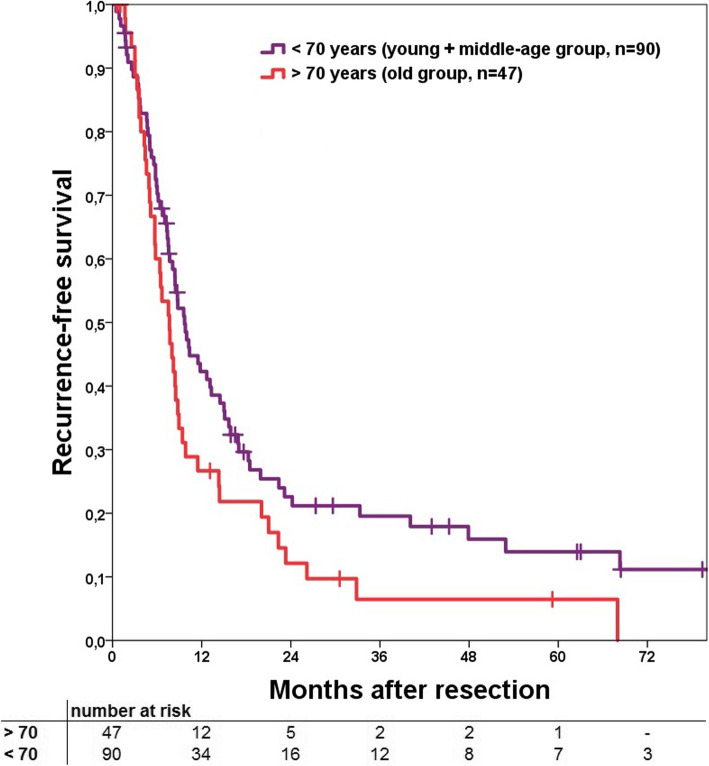
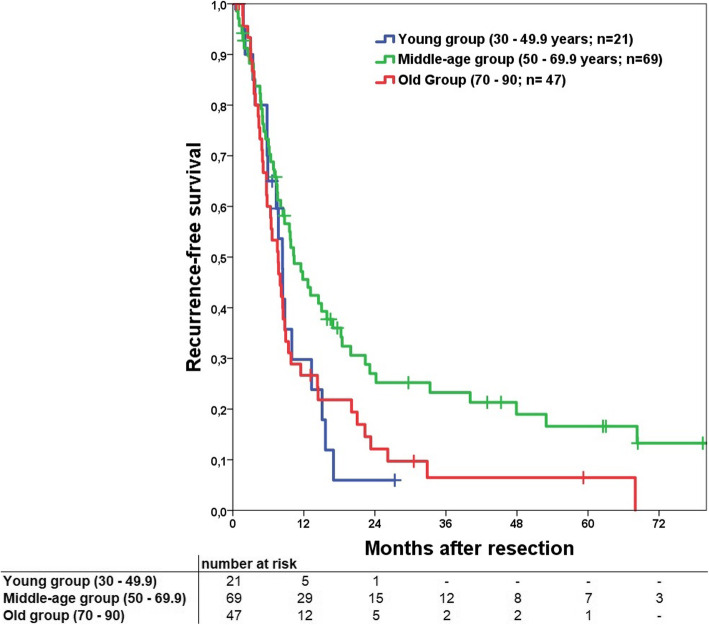
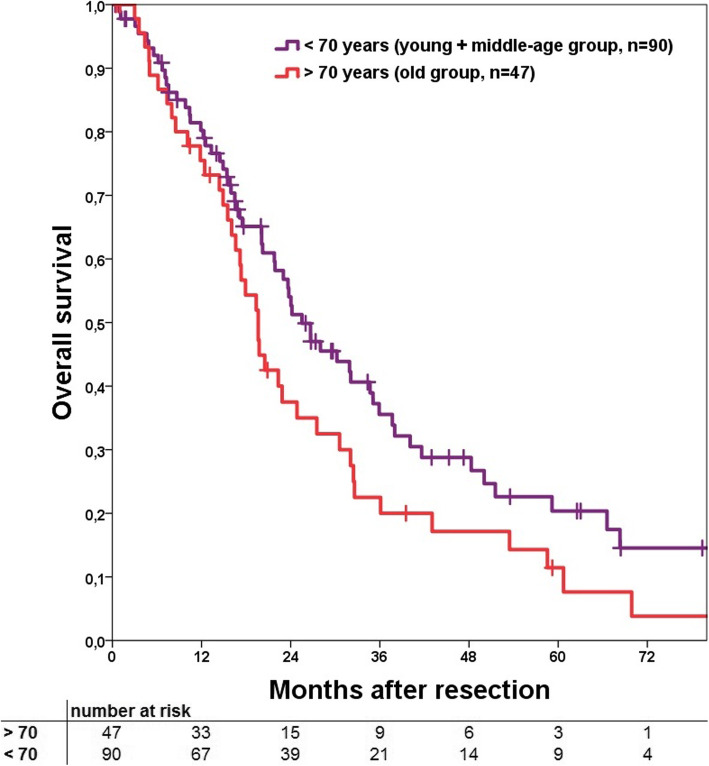
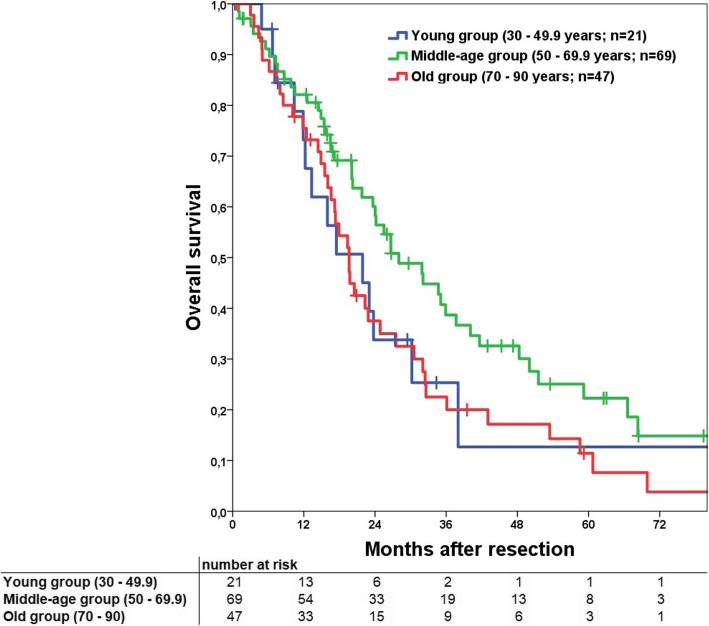
Results: In total 210 patients underwent surgical exploration with 150 resections (71.4%). Patients were divided in 70-years cut-off groups (> 70 vs < 70 years of age) as well as a young (age 30-50, n = 23), middle-age (50-70, n = 76) and old (> 70, n = 51) group, whose results are presented here. Resectability (p = 0.709), extent of surgery (p = 0.765), morbidity (p = 0.420) and mortality (p = 0.965) was comparable between the different age groups. Neither visceral (p = 0.991) nor vascular (p = 0.614) extension differed significantly, likewise tumor recurrence (p = 0.300) or the localisation of recurrence (p = 0.722). In comparison of patients > or < 70 years of age, recurrence-free survival (RFS) was significantly better for the younger group (p = 0.047). For overall survival (OS) a benefit could be shown, but without reaching significance (p = 0.072). In subgroup analysis the middle-age group had significant better OS (p = 0.020) and RFS (p = 0.038) compared to the old group. Additionally, a better OS (p = 0.076) and RFS (p = 0.179) was shown in comparison with the young group as well, but without reaching significance. The young compared to the old group had analogous OS (p = 0.931) and RFS (p = 0.845).
Conclusion: Resection of ICC in elderly patients is not associated with an increased perioperative risk. Even extended resections can be performed in elderly patients without obvious disadvantages. Middle-age patients have a clear benefit for OS and RFS, while young and old patients have a comparable and worse long-term outcome.
Keywords: Cholangiocarcinoma; Elderly; Geriatric; Intrahepatic cholangiocarcinoma; Liver surgery.
Conflict of interest statement
The authors declare that they have no financial or non-financial competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
