

A systematic review and meta-analysis of postpartum contraceptive use among women in low- and middle-income countries
- PMID: 31665032
- PMCID: PMC6819406
- DOI: 10.1186/s12978-019-0824-4
A systematic review and meta-analysis of postpartum contraceptive use among women in low- and middle-income countries
Abstract
Background: Short birth intervals increase risk for adverse maternal and infant outcomes including preterm birth, low birth weight (LBW), and infant mortality. Although postpartum family planning (PPFP) is an increasingly high priority for many countries, uptake and need for PPFP varies in low- and middle-income countries (LMIC). We performed a systematic review and meta-analysis to characterize postpartum contraceptive use, and predictors and barriers to use, among postpartum women in LMIC.
Methods: PubMed, EMBASE, CINAHL, PsycINFO, Scopus, Web of Science, and Global Health databases were searched for articles and abstracts published between January 1997 and May 2018. Studies with data on contraceptive uptake through 12 months postpartum in low- and middle-income countries were included. We used random-effects models to compute pooled estimates and confidence intervals of modern contraceptive prevalence rates (mCPR), fertility intentions (birth spacing and birth limiting), and unmet need for contraception in the postpartum period.
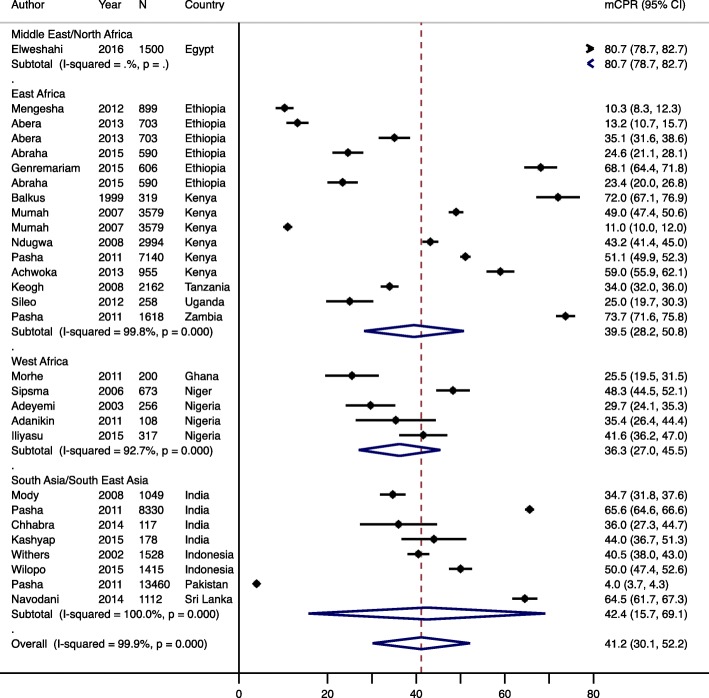
Results: Among 669 studies identified, 90 were selected for full-text review, and 35 met inclusion criteria. The majority of studies were from East Africa, West Africa, and South Asia/South East Asia. The overall pooled mCPR during the postpartum period across all regions was 41.2% (95% CI: 15.7-69.1%), with lower pooled mCPR in West Africa (36.3%; 95% CI: 27.0-45.5%). The pooled prevalence of unmet need was 48.5% (95% CI: 19.1-78.0%) across all regions, and highest in South Asia/South East Asia (59.4, 95% CI: 53.4-65.4%). Perceptions of low pregnancy risk due to breastfeeding and postpartum amenorrhea were commonly associated with lack of contraceptive use and use of male condoms, withdrawal, and abstinence. Women who were not using contraception were also less likely to utilize maternal and child health (MCH) services and reside in urban settings, and be more likely to have a fear of method side effects and receive inadequate FP counseling. In contrast, women who received FP counseling in antenatal and/or postnatal care were more likely to use PPFP.
Conclusions: PPFP use is low and unmet need for contraception following pregnancy in LMIC is high. Tailored counseling approaches may help overcome misconceptions and meet heterogeneous needs for PPFP.
Keywords: Barriers; Contraceptives; Low income; Middle income; Postpartum; Predictors.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures






Similar articles
-
Effect of integrating maternal health services and family planning services on postpartum family planning behavior in Ethiopia: results from a longitudinal survey.BMC Public Health. 2019 Nov 4;19(1):1448. doi: 10.1186/s12889-019-7703-3. BMC Public Health. 2019. PMID: 31684905 Free PMC article.
-
New IPPF statement on breastfeeding, fertility and post-partum contraception.IPPF Med Bull. 1990 Apr;24(2):2-4. IPPF Med Bull. 1990. PMID: 12316285
-
Increasing Use of Postpartum Family Planning and the Postpartum IUD: Early Experiences in West and Central Africa.Glob Health Sci Pract. 2016 Aug 18;4 Suppl 2(Suppl 2):S140-52. doi: 10.9745/GHSP-D-16-00039. Print 2016 Aug 11. Glob Health Sci Pract. 2016. PMID: 27540120 Free PMC article.
-
Effective strategies for increasing the uptake of modern methods of family planning in South Asia: a systematic review and meta-analysis.BMC Womens Health. 2024 Jan 3;24(1):13. doi: 10.1186/s12905-023-02859-2. BMC Womens Health. 2024. PMID: 38172863 Free PMC article.
-
Factors associated with modern contraceptives uptake during the first year after birth in Ethiopia: A systematic review and meta-analysis.PLoS One. 2023 Feb 7;18(2):e0270055. doi: 10.1371/journal.pone.0270055. eCollection 2023. PLoS One. 2023. PMID: 36749759 Free PMC article.
Cited by
-
mHealth interventions for postpartum family planning in LMICs: A realist review.PLOS Glob Public Health. 2024 Jul 18;4(7):e0003432. doi: 10.1371/journal.pgph.0003432. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 39024319 Free PMC article.
-
Exploration of modern contraceptive methods using patterns among later reproductive-aged women in Bangladesh.PLoS One. 2024 Apr 1;19(4):e0291100. doi: 10.1371/journal.pone.0291100. eCollection 2024. PLoS One. 2024. PMID: 38557777 Free PMC article.
-
Knowledge, Utilization and Associated Factors of Postpartum Family Planning Among Women Who Had Delivered a Baby in the Past Year in Oromia Regional State, Ethiopia.Open Access J Contracept. 2020 Oct 22;11:167-176. doi: 10.2147/OAJC.S268561. eCollection 2020. Open Access J Contracept. 2020. PMID: 33116967 Free PMC article.
-
Effects of maternal healthcare service utilization on modern postpartum family planning access in Bangladesh: insights from a National representative survey.PLoS One. 2025 Feb 4;20(2):e0318363. doi: 10.1371/journal.pone.0318363. eCollection 2025. PLoS One. 2025. PMID: 39903768 Free PMC article.
-
Expanding access to postpartum contraception.Curr Opin Obstet Gynecol. 2024 Oct 1;36(5):331-337. doi: 10.1097/GCO.0000000000000982. Epub 2024 Aug 2. Curr Opin Obstet Gynecol. 2024. PMID: 39109628 Free PMC article. Review.
References
-
- Marston C. Report of a WHO technical consultation on birth spacing Geneva Switzerland 13–15 June 2005. 2006.
-
- WHO: Postpartum family planning: essential for ensuring health of women and their babies. World Contraception Day 2018. Accessed on 13 Sept 2019 at https://www.who.int/reproductivehealth/topics/family_planning/world-cont....
-
- WHO: Programming strategies for postpartum family planning. ISBN 978 92 4 150649 6 (NLM classification: WA 550). Geneva: World Health Organization. 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
