

Biomarkers and clinical scores to identify patient populations at risk of delayed antibiotic administration or intensive care admission
- PMID: 31665092
- PMCID: PMC6819475
- DOI: 10.1186/s13054-019-2613-4
Biomarkers and clinical scores to identify patient populations at risk of delayed antibiotic administration or intensive care admission
Abstract
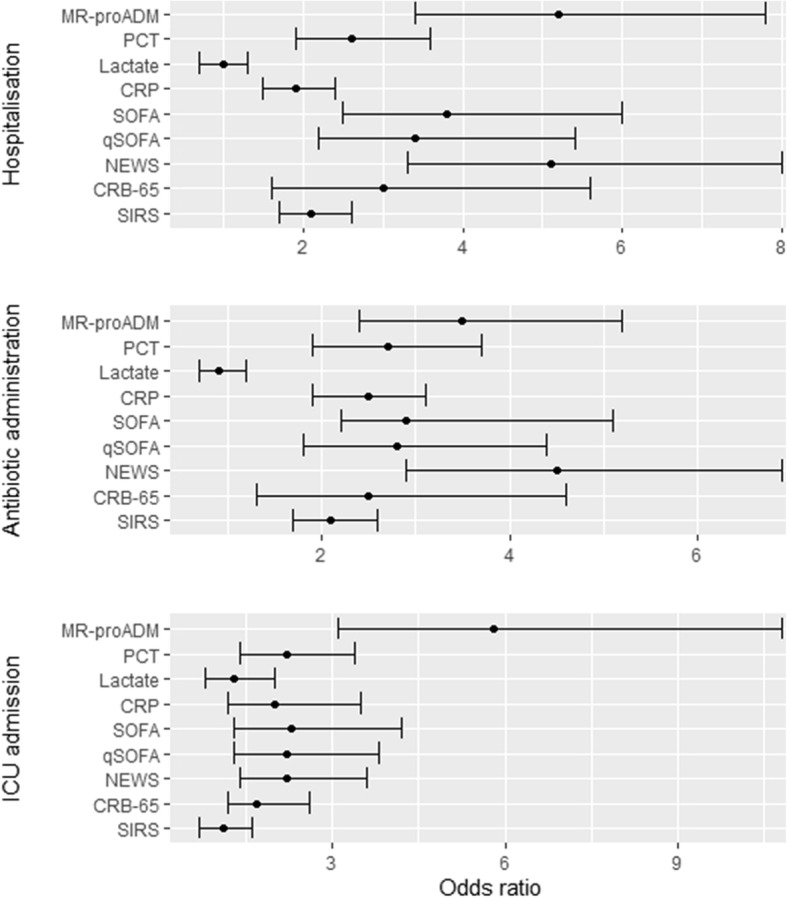
Background: The performance of blood biomarkers (mid-regional proadrenomedullin (MR-proADM), procalcitonin (PCT), C-reactive protein (CRP), and lactate) and clinical scores (Sequential Organ Failure Assessment (SOFA), National Early Warning Score (NEWS), and quick SOFA) was compared to identify patient populations at risk of delayed treatment initiation and disease progression after presenting to the emergency department (ED) with a suspected infection.
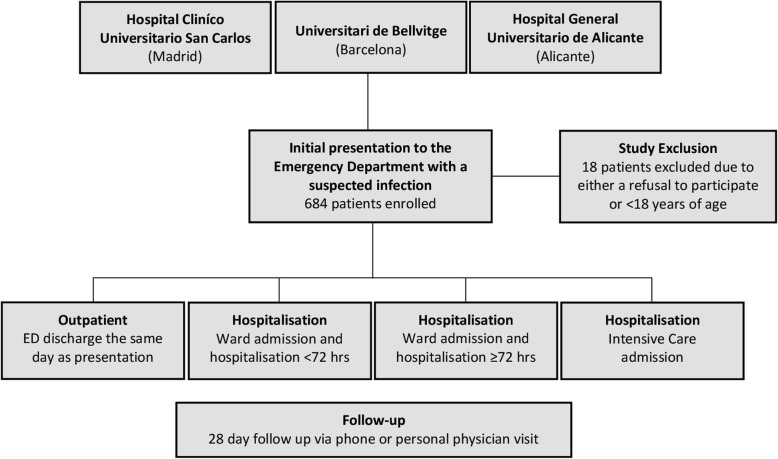
Methods: A prospective observational study across three EDs. Biomarker and clinical score values were calculated upon presentation and 72 h, and logistic and Cox regression used to assess the strength of association. Primary outcomes comprised of 28-day mortality prediction and delayed antibiotic administration or intensive care (ICU) admission, whilst secondary outcomes identified subsequent disease progression.
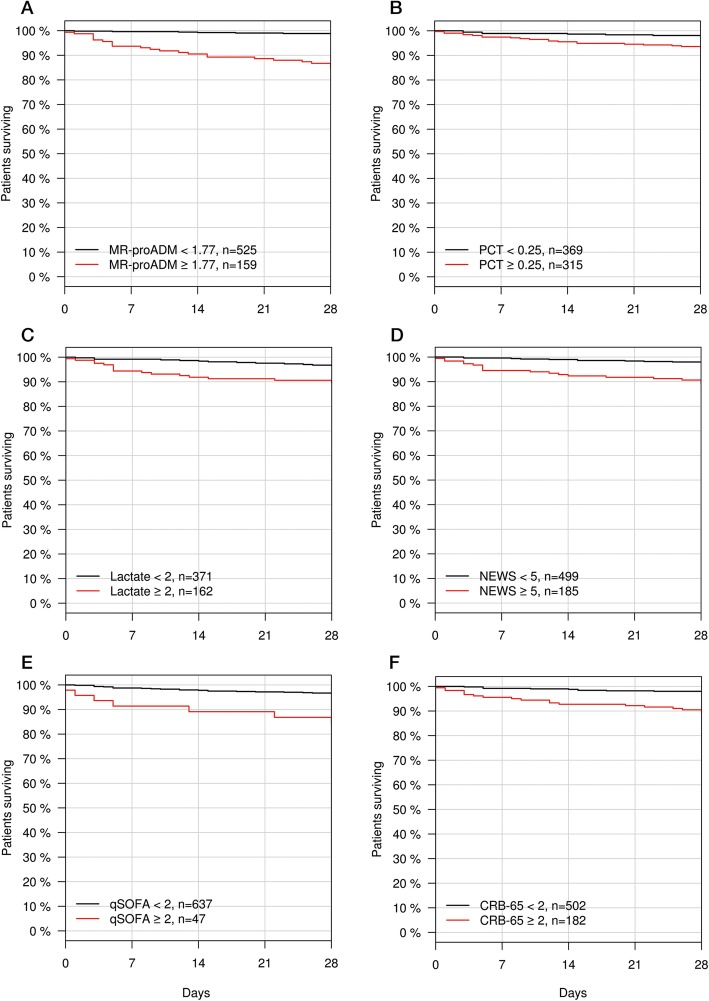
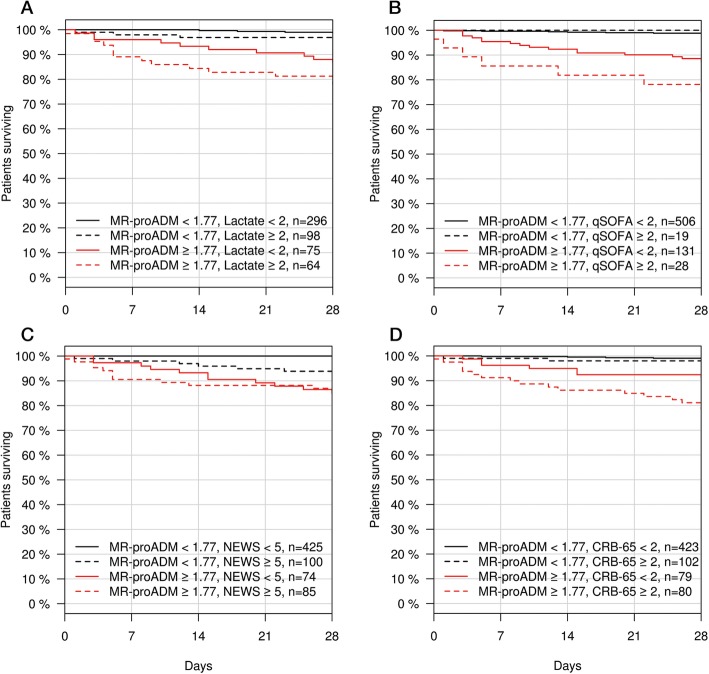
Results: Six hundred eighty-four patients were enrolled with hospitalisation, ICU admission, and infection-related 28-day mortality rates of 72.8%, 3.4%, and 4.4%, respectively. MR-proADM and NEWS had the strongest association with hospitalisation and the requirement for antibiotic administration, whereas MR-proADM alone had the strongest association with ICU admission (OR [95% CI]: 5.8 [3.1 - 10.8]) and mortality (HR [95% CI]: 3.8 [2.2 - 6.5]). Patient subgroups with high MR-proADM concentrations (≥ 1.77 nmol/L) and low NEWS (< 5 points) values had significantly higher rates of ICU admission (8.1% vs 1.6%; p < 0.001), hospital readmission (18.9% vs. 5.9%; p < 0.001), infection-related mortality (13.5% vs. 0.2%; p < 0.001), and disease progression (29.7% vs. 4.9%; p < 0.001) than corresponding patients with low MR-proADM concentrations. ICU admission was delayed by 1.5 [0.25 - 5.0] days in patients with high MR-proADM and low NEWS values compared to corresponding patients with high NEWS values, despite similar 28-day mortality rates (13.5% vs. 16.5%). Antibiotics were withheld in 17.4% of patients with high MR-proADM and low NEWS values, with higher subsequent rates of ICU admission (27.3% vs. 4.8%) and infection-related hospital readmission (54.5% vs. 14.3%) compared to those administered antibiotics during ED treatment.
Conclusions: Patients with low severity signs of infection but high MR-proADM concentrations had an increased likelihood of subsequent disease progression, delayed antibiotic administration or ICU admission. Appropriate triage decisions and the rapid use of antibiotics in patients with high MR-proADM concentrations may constitute initial steps in escalating or intensifying early treatment strategies.
Keywords: Disease progression; Emergency department; Infection; Intensive care unit; MR-proADM; NEWS; Sepsis; qSOFA.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Gaieski DF, Mikkelsen ME, Band RA, Pines JM, Massone R, Furia FF, et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department*. Crit Care Med. 2010;38(4):1045–1053. doi: 10.1097/CCM.0b013e3181cc4824. - DOI - PubMed
-
- Saeed K, Wilson DC, Bloos F, Schuetz P, van der Does Y, Melander O, et al. The early identification of disease progression in patients with suspected infection presenting to the emergency department: a multi-centre derivation and validation study. Crit Care. 2019;23(1):40. doi: 10.1186/s13054-019-2329-5. - DOI - PMC - PubMed
-
- Stalenhoef JE, Nieuwkoop C, Wilson DC, Starre WE, Delfos NM, Leyten EMS, et al. Biomarker guided traige can reduce hospitalisation rate in community acquired febrile urinary tract infection. J Infect. 2018;77(1):18–24. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
