

Cumulative fluid balance predicts mortality and increases time on mechanical ventilation in ARDS patients: An observational cohort study
- PMID: 31665179
- PMCID: PMC6821102
- DOI: 10.1371/journal.pone.0224563
Cumulative fluid balance predicts mortality and increases time on mechanical ventilation in ARDS patients: An observational cohort study
Abstract
Introduction: Acute respiratory distress syndrome (ARDS) is characterized by acute, diffuse, inflammatory lung injury leading to increased pulmonary vascular permeability, pulmonary oedema and loss of aerated tissue. Previous literature showed that restrictive fluid therapy in ARDS shortens time on mechanical ventilation and length of ICU-stay. However, the effect of intravenous fluid use on mortality remains uncertain. We investigated the relationship between cumulative fluid balance (FB), time on mechanical ventilation and mortality in ARDS patients.
Materials and methods: Retrospective observational study. Patients were divided in four cohorts based on cumulative FB on day 7 of ICU-admission: ≤0 L (Group I); 0-3.5 L (Group II); 3.5-8 L (Group III) and ≥8 L (Group IV). In addition, we used cumulative FB on day 7 as continuum as a predictor of mortality. Primary outcomes were 28-day mortality and ventilator-free days. Secondary outcomes were 90-day mortality and ICU length of stay.
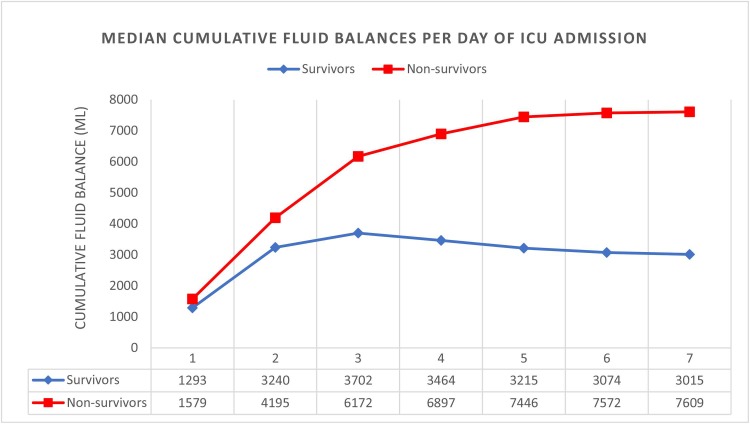
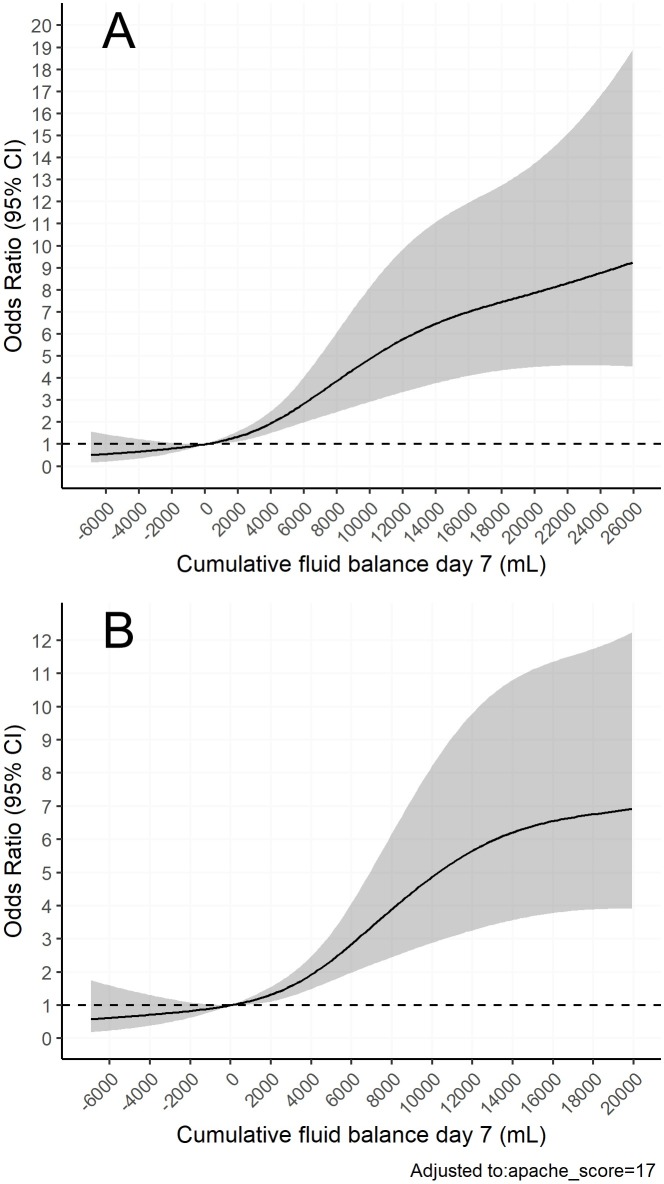
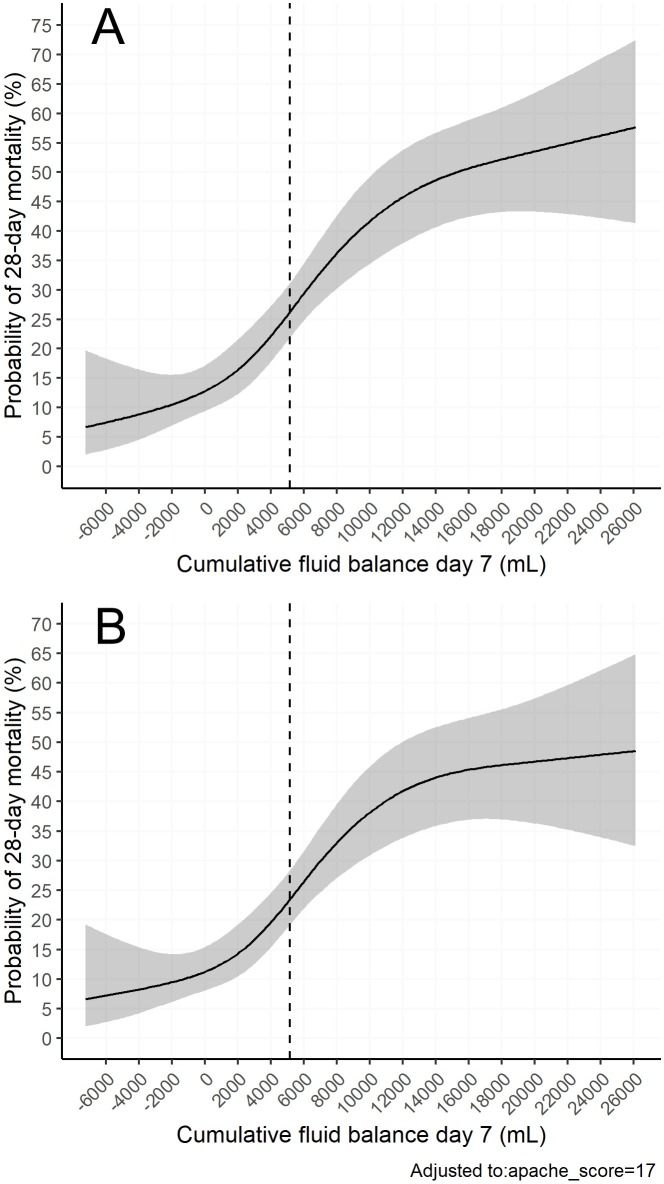
Results: Six hundred ARDS patients were included, of whom 156 (26%) died within 28 days. Patients with a higher cumulative FB on day 7 had a longer length of ICU-stay and fewer ventilator-free days on day 28. Furthermore, after adjusting for severity of illness, a higher cumulative FB was associated with 28-day mortality (Group II, adjusted OR (aOR) 2.1 [1.0-4.6], p = 0.045; Group III, aOR 3.3 [1.7-7.2], p = 0.001; Group IV, aOR 7.9 [4.0-16.8], p<0.001). Using restricted cubic splines, a non-linear dose-response relationship between cumulative FB and probability of death at day 28 was found; where a more positive FB predicted mortality and a negative FB showed a trend towards survival.
Conclusions: A higher cumulative fluid balance is independently associated with increased risk of death, longer time on mechanical ventilation and longer length of ICU-stay in patients with ARDS. This underlines the importance of implementing restrictive fluid therapy in ARDS patients.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Malbrain ML, Marik PE, Witters I, Cordemans C, Kirkpatrick AW, Roberts DJ, et al. Fluid overload, de-resuscitation, and outcomes in critically ill or injured patients: a systematic review with suggestions for clinical practice. Anaesthesiol Intensive Ther. 2014;46(5):361–80. Epub 2014/11/30. 10.5603/AIT.2014.0060 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
