

Prospective comparison of two enzyme-linked immunosorbent spot assays for the diagnosis of Lyme neuroborreliosis
- PMID: 31665540
- PMCID: PMC7008225
- DOI: 10.1111/cei.13393
Prospective comparison of two enzyme-linked immunosorbent spot assays for the diagnosis of Lyme neuroborreliosis
Abstract
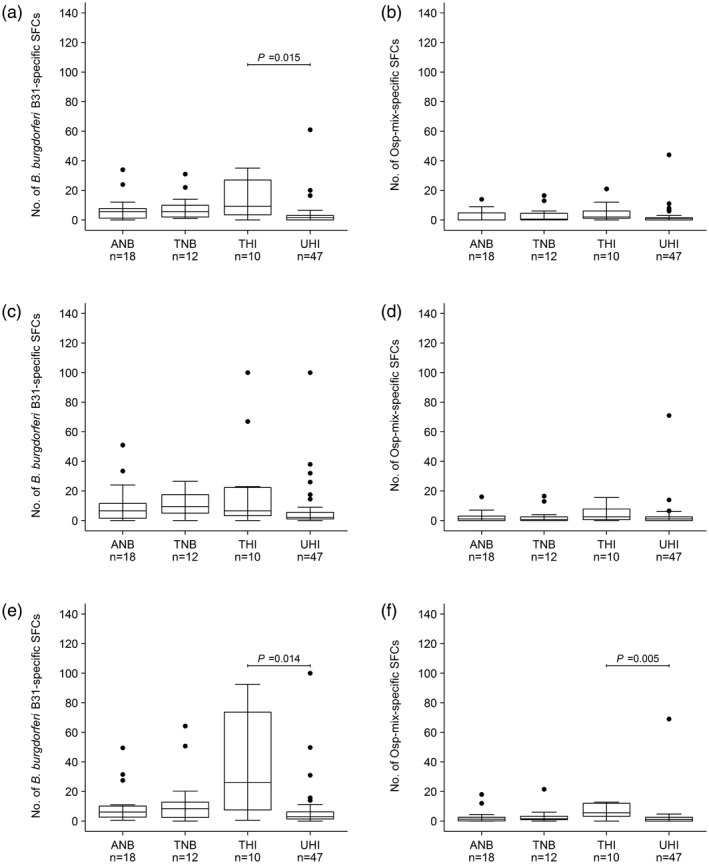
Commercial cellular tests are used to diagnose Lyme borreliosis (LB), but studies on their clinical validation are lacking. This study evaluated the utility of an in-house and a commercial enzyme-linked immunosorbent spot (ELISpot) assay for the diagnosis of Lyme neuroborreliosis (LNB). Prospectively, peripheral blood mononuclear cells (PBMCs) were isolated from patients and controls and analysed using an in-house Borrelia ELISpot assay and the commercial LymeSpot assay. B. burgdorferi B31 whole cell lysate and a mixture of outer surface proteins were used to stimulate the PBMCs and the numbers of interferon-gamma-secreting T cells were measured. Results were evaluated using receiver operating characteristic (ROC) curve analysis. Eighteen active and 12 treated LNB patients, 10 healthy individuals treated for an early (mostly cutaneous) manifestation of LB in the past and 47 untreated healthy individuals were included. Both assays showed a poor diagnostic performance with sensitivities, specificities, positive and negative predictive values ranging from 44.4-66.7%, 42.0-72.5%, 21.8-33.3% and 80.5-87.0%, respectively. The LymeSpot assay performed equally poorly when the calculation method of the manufacturer was used. Both the in-house and the LymeSpot assay are unable to diagnose active LNB or to monitor antibiotic treatment success.
Keywords: Borrelia; ELISpot; Lyme neuroborreliosis; T cells; interferon-gamma.
© 2019 The Authors. Clinical & Experimental Immunology published by John Wiley & Sons Ltd on behalf of British Society for Immunology.
Conflict of interest statement
None.
Figures

Comment in
-
ELISPOT assays and their diagnostic potential in Lyme disease and Lyme neuroborreliosis.Clin Exp Immunol. 2020 Jun;200(3):299-301. doi: 10.1111/cei.13431. Epub 2020 Apr 14. Clin Exp Immunol. 2020. PMID: 32180218 Free PMC article. No abstract available.
References
-
- National Institute for Public Health and the Environment, the Netherlands . Lyme disease cases have quadrupled. Available at: https://www.rivm.nl/en/Documents_and_publications/Common_and_Present/New... (Accessed June 2018).
-
- de Mik EL, van Pelt W, Docters‐van Leeuwen BD, van der Veen A, Schellekens JF, Borgdorff MW. The geographical distribution of tick bites and erythema migrans in general practice in the Netherlands. Int J Epidemiol 1997; 26:451–7. - PubMed
-
- Kwaliteitsinstituut voor de Gezondheidszorg (CBO) . [CBO‐richtlijn Lymeziekte definitief]. 2013. Available at: https://www.rivm.nl/nieuws/cbo-richtlijn-lymeziekte-definitief (Accessed June 2018).
-
- Wilske B. Diagnosis of Lyme borreliosis in Europe. Vector‐Borne Zoonot. Dis 2003; 3:215–27. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
