

Predictive and diagnostic biomarkers for gestational diabetes and its associated metabolic and cardiovascular diseases
- PMID: 31666083
- PMCID: PMC6820966
- DOI: 10.1186/s12933-019-0935-9
Predictive and diagnostic biomarkers for gestational diabetes and its associated metabolic and cardiovascular diseases
Abstract
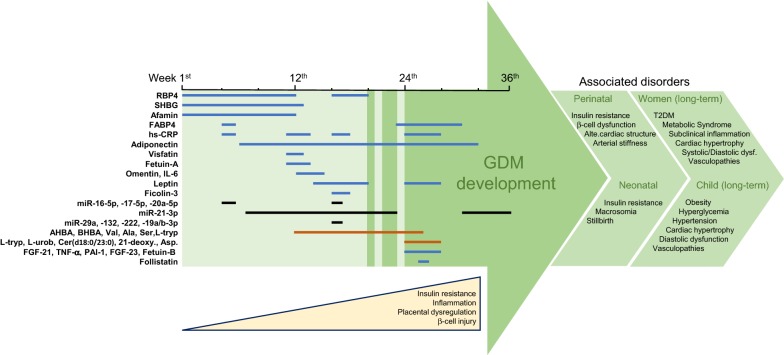
Gestational diabetes mellitus (GDM) is defined as the presence of high blood glucose levels with the onset, or detected for the first time during pregnancy, as a result of increased insulin resistance. GDM may be induced by dysregulation of pancreatic β-cell function and/or by alteration of secreted gestational hormones and peptides related with glucose homeostasis. It may affect one out of five pregnancies, leading to perinatal morbidity and adverse neonatal outcomes, and high risk of chronic metabolic and cardiovascular injuries in both mother and offspring. Currently, GDM diagnosis is based on evaluation of glucose homeostasis at late stages of pregnancy, but increased age and body-weight, and familiar or previous occurrence of GDM, may conditionate this criteria. In addition, an earlier and more specific detection of GDM with associated metabolic and cardiovascular risk could improve GDM development and outcomes. In this sense, 1st-2nd trimester-released biomarkers found in maternal plasma including adipose tissue-derived factors such as adiponectin, visfatin, omentin-1, fatty acid-binding protein-4 and retinol binding-protein-4 have shown correlations with GDM development. Moreover, placenta-related factors such as sex hormone-binding globulin, afamin, fetuin-A, fibroblast growth factors-21/23, ficolin-3 and follistatin, or specific micro-RNAs may participate in GDM progression and be useful for its recognition. Finally, urine-excreted metabolites such as those related with serotonin system, non-polar amino-acids and ketone bodies, may complete a predictive or early-diagnostic panel of biomarkers for GDM.
Keywords: Cardiovascular disease; Diagnostic biomarkers; Gestational diabetes; Metabolic disease; Predictive biomarkers.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
