

High sdLDL Cholesterol can be Used to Reclassify Individuals with Low Cardiovascular Risk for Early Intervention: Findings from the Chinese Multi-Provincial Cohort Study
- PMID: 31666437
- PMCID: PMC7406409
- DOI: 10.5551/jat.49841
High sdLDL Cholesterol can be Used to Reclassify Individuals with Low Cardiovascular Risk for Early Intervention: Findings from the Chinese Multi-Provincial Cohort Study
Abstract
Aim: A high-risk strategy has been implemented for lipid-lowering therapy in the primary prevention of cardiovascular disease. However, atherosclerosis and cardiovascular events are common among individuals with low cardiovascular risk. This study aimed to determine whether the small dense low-density lipoprotein cholesterol (sdLDLC) level can predict carotid atherosclerosis progression and identify high-risk individuals.
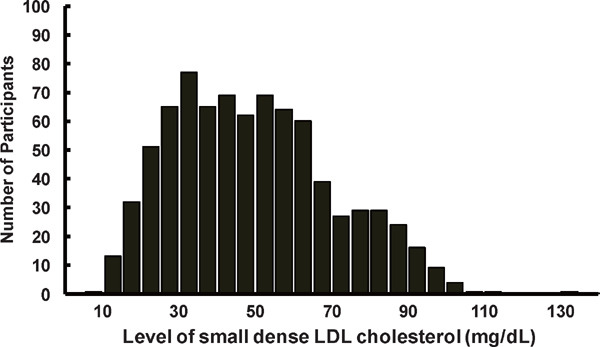
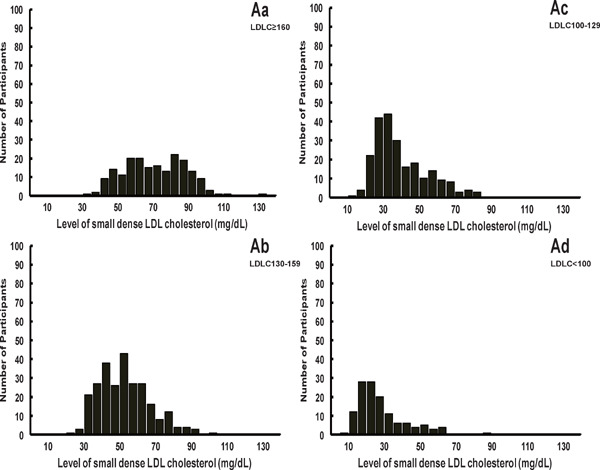
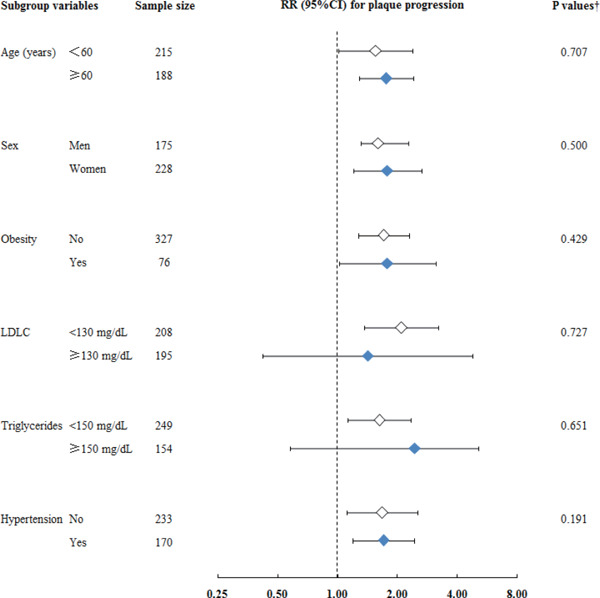
Methods: Baseline sdLDLC and low-density lipoprotein cholesterol (LDLC) were measured in 808 participants from the Chinese Multi-provincial Cohort Study, aged 45-74 years. Adjusted relative risk was calculated using a modified Poisson regression model to assess the relationship between sdLDLC and 5-year atherosclerosis progression, as indicated by the progression, incidence, and multi-territorial extent of carotid plaque.
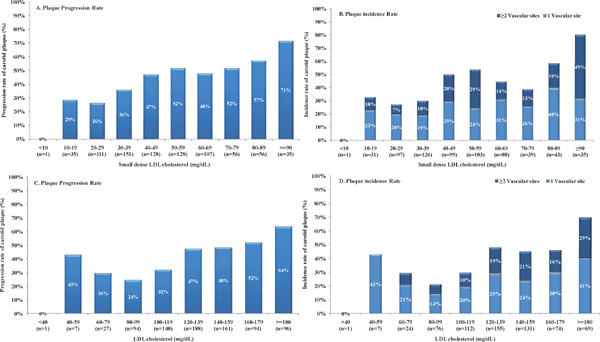
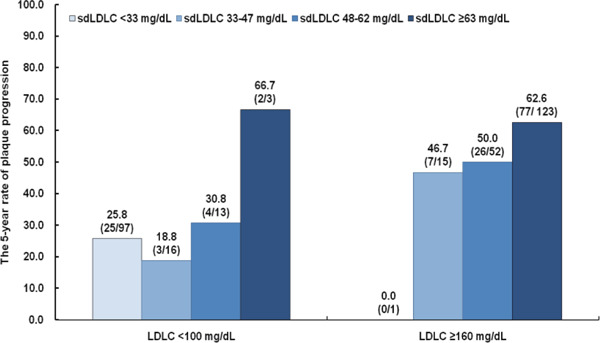
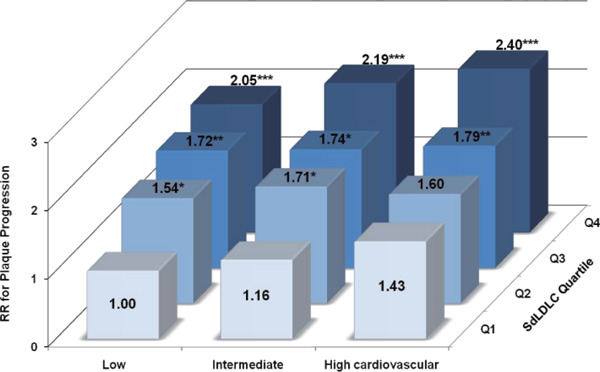
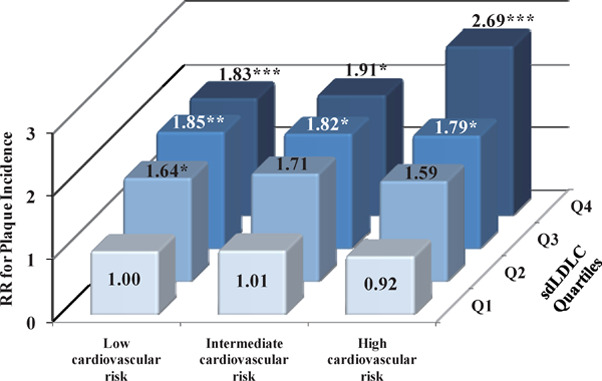
Results: The 5-year atherosclerosis progression increased significantly with increased sdLDLC. Baseline sdLDLC was significantly associated with the short-term risk of plaque progression after multivariable adjustment, even in participants with low LDLC or a 10-year estimated cardiovascular risk. sdLDLC predicted plaque progression (relative risk 2.05; 95% confidence interval 1.43-2.93) in participants with LDLC <130 mg/dL. Furthermore, participants with the highest sdLDLC but intermediate or low cardiovascular risk (accounting for 16% of the cohort) had double the risk of plaque progression, which was comparable to those with the same sdLDLC and high cardiovascular risk, relative to those with the lowest sdLDLC levels and low cardiovascular risk.
Conclusions: sdLDLC is independently associated with the progression of carotid atherosclerosis, which may provide a basis for clinicians to reclassify individuals believed to be at low cardiovascular risk into the high-risk category, and those with high sdLDLC may benefit from more aggressive cholesterol-lowering treatment.
Keywords: Carotid atherosclerosis; Community-based cohort study; High-risk strategy; Risk reclassification; Small dense low-density lipoprotein cholesterol.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this work.
Figures
References
-
- Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, Hoes AW, Jennings CS, Landmesser U, Pedersen TR, Reiner Z, Riccardi G, Taskinen MR, Tokgozoglu L, Monique Verschuren WM, Vlachopoulos C, Wood DA, Luis Zamorano J, Cooney MT: 2016 ESC/EAS guidelines for the management of dyslipidaemias. Rev Esp Cardiol (Engl Ed), 2017; 70: 115. - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella-Tommasino J, Forman DE, Goldberg R, Heidenreich PA, Hlatky MA, Jones DW, Lloyd-Jones D, Lopez-Pajares N, Ndumele CE, Orringer CE, Peralta CA, Saseen JJ, Smith SC, Jr., Sperling L, Virani SS, Yeboah J: 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the american college of cardiology/american heart association task force on clinical practice guidelines. J Am Coll Cardiol, 2019; 73: e285-e350 - PubMed
-
- Zhang M, Deng Q, Wang L, Huang Z, Zhou M, Li Y, Zhao Z, Zhang Y: Prevalence of dyslipidemia and achievement of low-density lipoprotein cholesterol targets in chinese adults: a nationally representative survey of 163,641 adults. Int J Cardiol, 2018; 260: 196-203 - PubMed
-
- Fernandez-Friera L, Fuster V, Lopez-Melgar B, Oliva B, Garcia-Ruiz JM, Mendiguren J, Bueno H, Pocock S, Ibanez B, Fernandez-Ortiz A, Sanz J: Normal ldl-cholesterol levels are associated with subclinical atherosclerosis in the absence of risk factors. J Am Coll Cardiol, 2017; 70: 2979-2991 - PubMed