

Postoperative Hypoparathyroidism in Thyroid Surgery: Anatomic-Surgical Mapping of the Parathyroids and Implications for Thyroid Surgery
- PMID: 31666619
- PMCID: PMC6821921
- DOI: 10.1038/s41598-019-52189-3
Postoperative Hypoparathyroidism in Thyroid Surgery: Anatomic-Surgical Mapping of the Parathyroids and Implications for Thyroid Surgery
Abstract
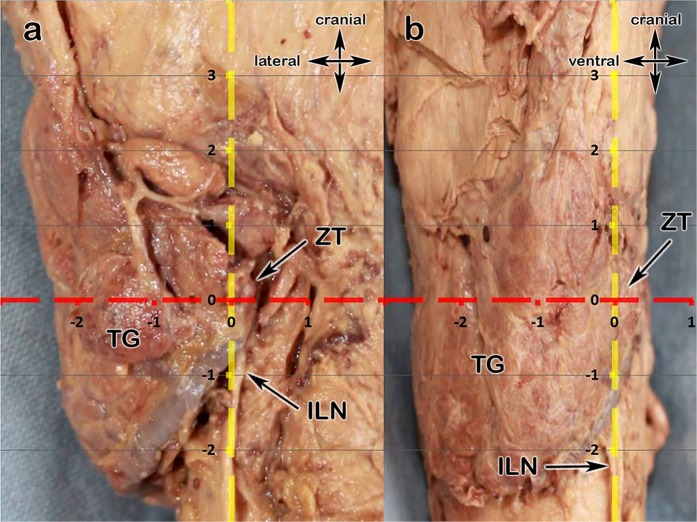
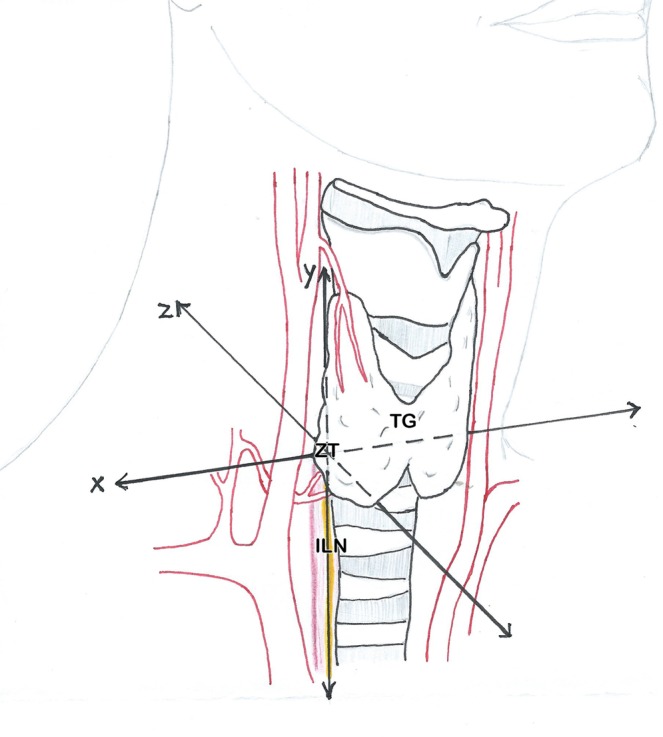
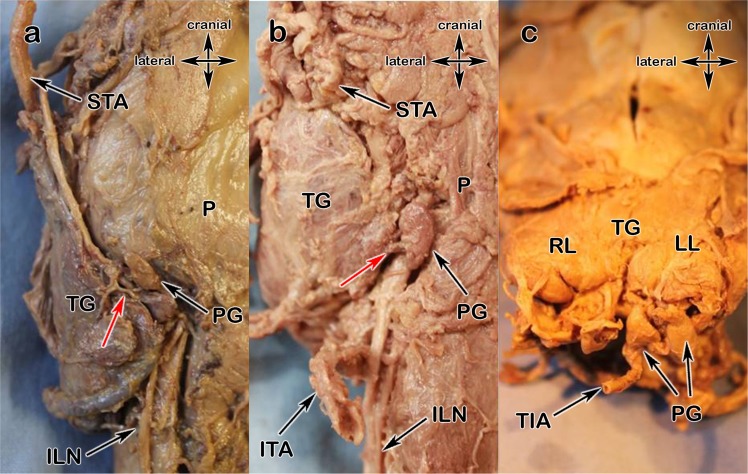
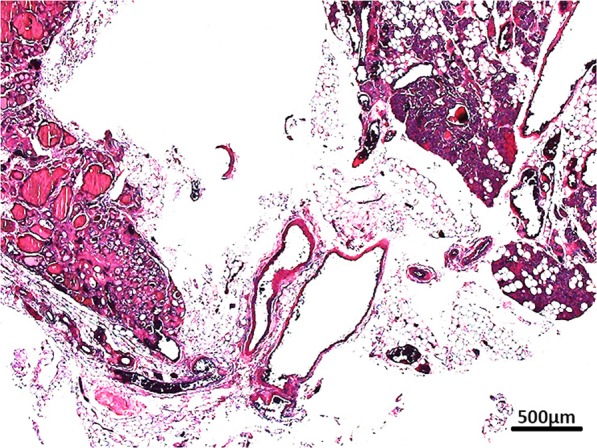
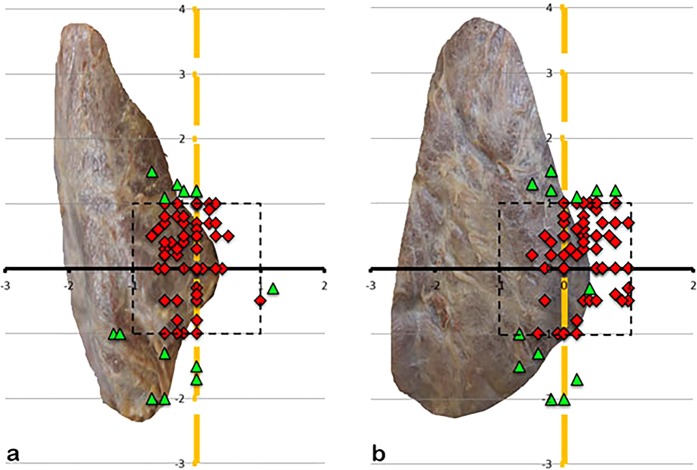
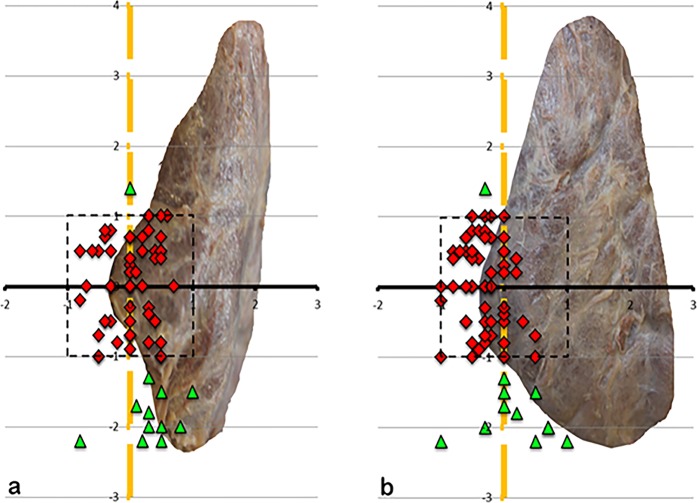
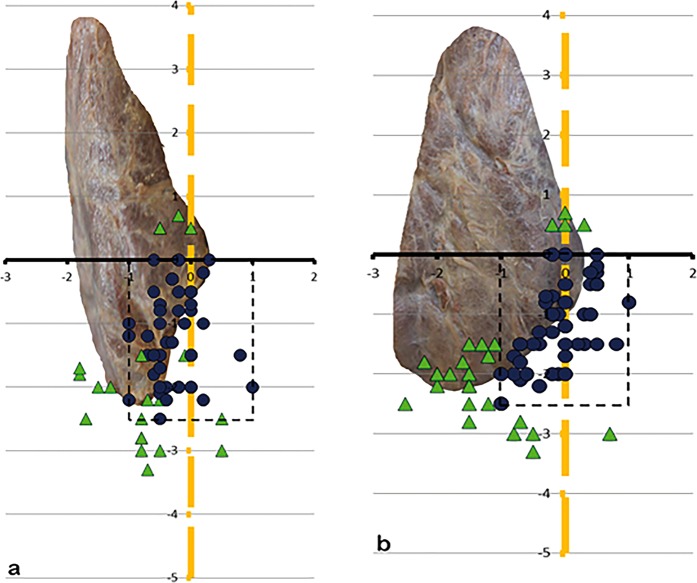
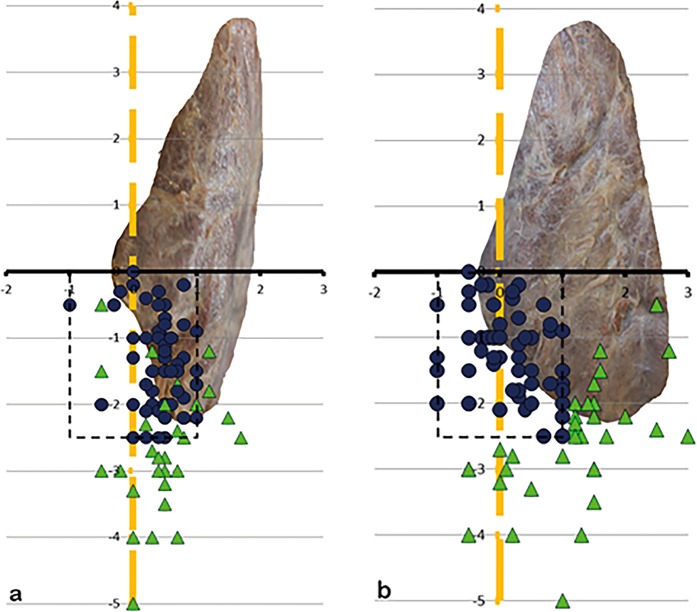
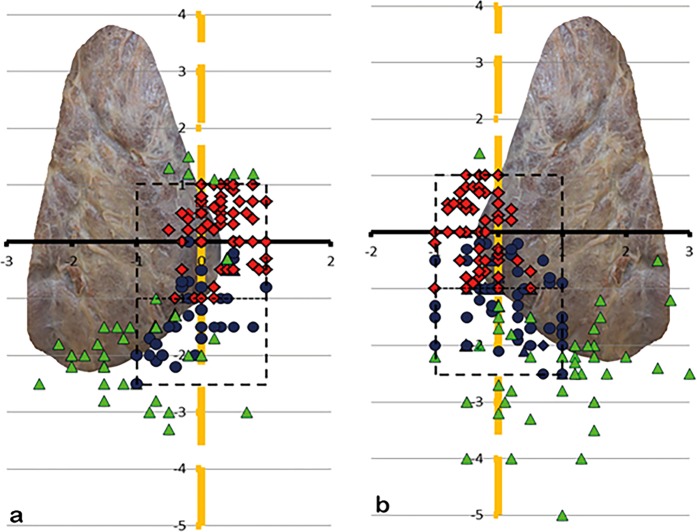
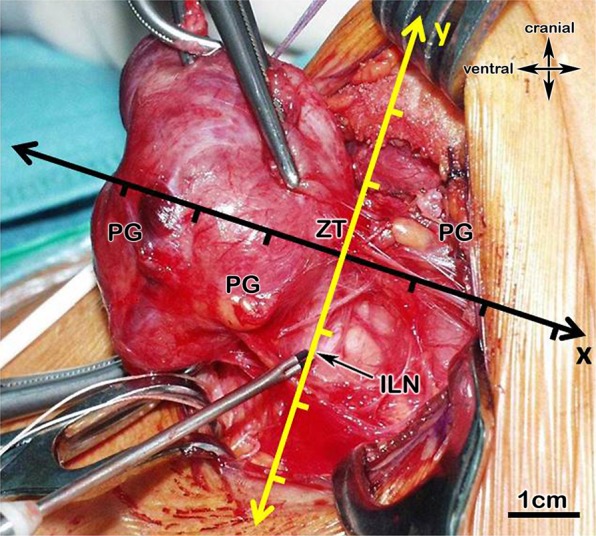
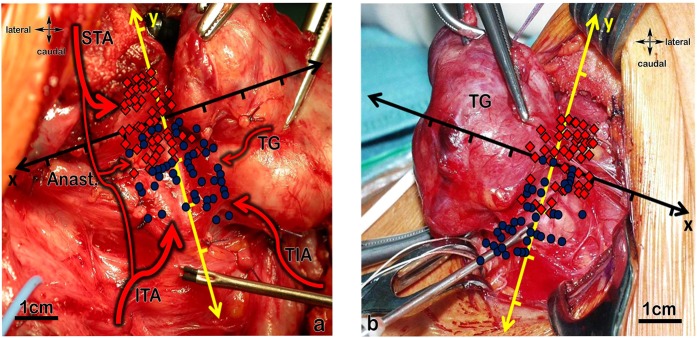
Hypoparathyroidism remains one of the most common complications in thyroid surgery. This study aims for an improved understanding of the complexity of the blood supply and the localisation of the parathyroids compared to the two most important intraoperative landmarks: the inferior laryngeal nerve (ILN) and Zuckerkandl's tubercle (ZT). We examined 103 laryngeal compounds to classify the blood supply and the localisation of the parathyroids. For intraoperative localisation we defined a Cartesian coordinate system with the ZT plane as x-axis and the course of the inferior laryngeal nerve as y-axis. The inferior thyroid artery (ITA) mainly supplies the parathyroids, whereas the superior thyroid artery provides a backup supply. It must be pointed out that 8.2% of parathyroids receive their blood directly from the thyroid gland. 73.5% of all parathyroids lie within 1 cm of the ILN and 1 cm cranial and 2.5 cm caudal to the ZT plane. Our described perimeters mark the most crucial areas during surgery and provide the surgeon with an anatomic mapping showing areas of special carefulness needed. One should keep bearing in mind all possible blood supply types of the parathyroids and therefore all branches should be handled with care.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Trupka, A. & Wicke, C. Nebenschilddrüsenprotektion zur Vermeidung des postoperativen Hypoparathyreoidismus. Dralle H. Endokrine Chirurgie-Evidenz und Erfahrung. Stuttgart: Schattauer, 117–136 (2014).
MeSH terms
LinkOut - more resources
Full Text Sources
