

Neoadjuvant therapy versus upfront surgery in resectable pancreatic cancer according to intention-to-treat and per-protocol analysis: A systematic review and meta-analysis
- PMID: 31666626
- PMCID: PMC6821820
- DOI: 10.1038/s41598-019-52167-9
Neoadjuvant therapy versus upfront surgery in resectable pancreatic cancer according to intention-to-treat and per-protocol analysis: A systematic review and meta-analysis
Abstract
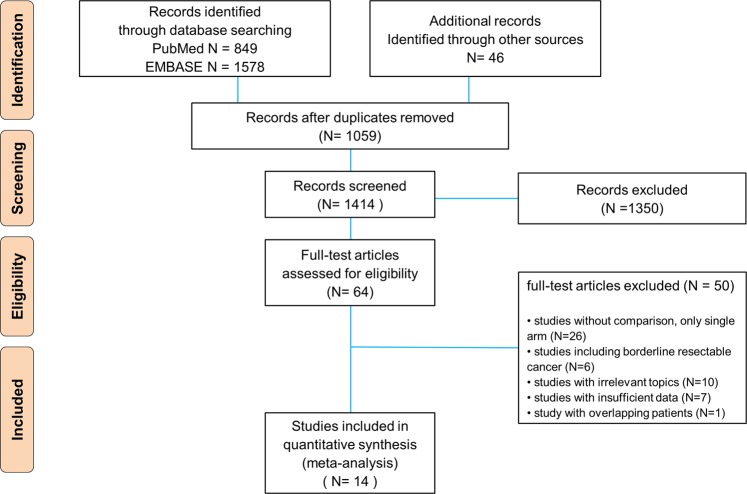
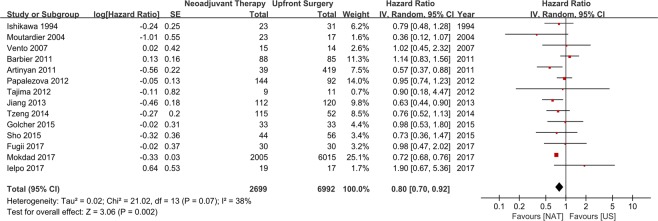
The effectiveness of neoadjuvant therapy (NAT) remains unclear in resectable pancreatic cancer (PC) as compared with upfront surgery (US). The aim of this study was to investigate the survival gain of NAT over US in resectable PC. PubMed and EMBASE were searched for studies comparing survival outcomes between NAT and US for resectable PC until June 2018. Overall survival (OS) was analyzed according to treatment strategy (NAT versus US) and analytic methods (intention-to-treat analysis (ITT) and per-protocol analysis (PP)). In 14 studies, 2,699 and 6,992 patients were treated with NAT and US, respectively. Although PP analysis showed the survival gain of NAT (HR 0.72, 95% CI 0.68-0.76), ITT analysis did not show the statistical significance (HR 0.96, 95% CI 0.82-1.12). However, NAT completed with subsequent surgery showed better survival over US completed with adjuvant therapy (HR 0.82, 95% CI 0.71-0.93). In conclusion, the supporting evidence for NAT in resectable PC was insufficient because the benefit was not demonstrated in ITT analysis. However, among the patients who completed both surgery and chemotherapy, NAT showed survival benefit over adjuvant therapy. Therefore, NAT could have a role of triaging the patients for surgery even in resectable PC.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Jang JY, et al. Oncological Benefits of Neoadjuvant Chemoradiation With Gemcitabine Versus Upfront Surgery in Patients With Borderline Resectable Pancreatic Cancer: A Prospective, Randomized, Open-label, Multicenter Phase 2/3 Trial. Ann Surg. 2018;268:215–222. doi: 10.1097/SLA.0000000000002705. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
