

The Population Impact of Late Presentation With Advanced HIV Disease and Delayed Antiretroviral Therapy in Adults Receiving HIV Care in Latin America
- PMID: 31667488
- PMCID: PMC7443201
- DOI: 10.1093/aje/kwz252
The Population Impact of Late Presentation With Advanced HIV Disease and Delayed Antiretroviral Therapy in Adults Receiving HIV Care in Latin America
Abstract
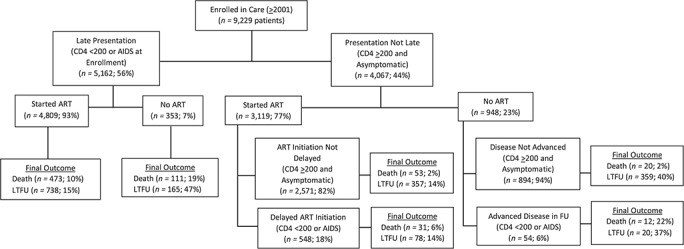
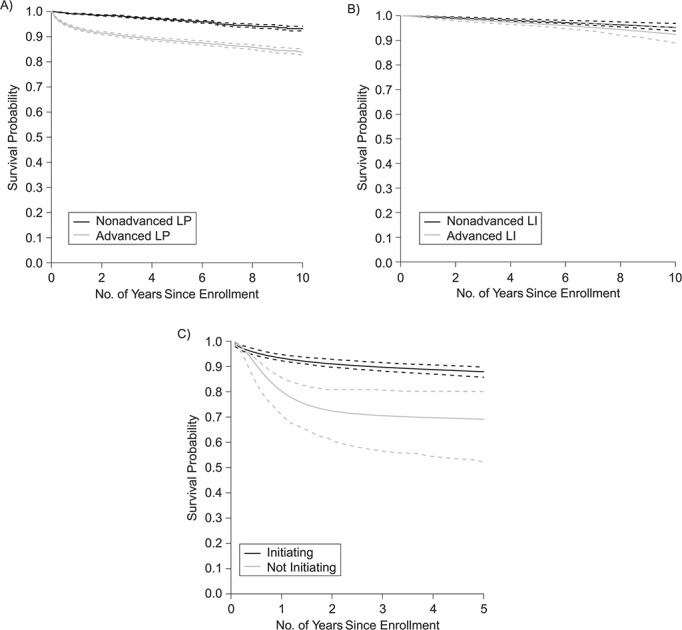
Late presentation to care and antiretroviral therapy (ART) initiation with advanced human immunodeficiency virus (HIV) disease are common in Latin America. We estimated the impact of these conditions on mortality in the region. We included adults enrolled during 2001-2014 at HIV care clinics. We estimated the adjusted attributable risk (AR) and population attributable fraction (PAF) for all-cause mortality of presentation to care with advanced HIV disease (advanced LP), ART initiation with advanced HIV disease, and not initiating ART. Advanced HIV disease was defined as CD4 of <200 cells/μL or acquired immune deficiency syndrome. AR and PAF were derived using marginal structural models. Of 9,229 patients, 56% presented with advanced HIV disease. ARs of death for advanced LP were 86%, 71%, and 58%, and PAFs were 78%, 58%, and 43% at 1, 5, and 10 years after enrollment. Among people without advanced LP, ARs of death for delaying ART were 39%, 32%, and 37% at 1, 5, and 10 years post-enrollment and PAFs were 20%, 14%, and 15%. Among people with advanced LP, ART decreased the hazard of death by 63% in the first year after enrollment, but 93% of these started ART; thus universal ART among them would reduce mortality by only 10%. Earlier presentation to care and earlier ART initiation would prevent most HIV deaths in Latin America.
Keywords: HIV infection; Latin America; acquired immune deficiency syndrome; adult; early diagnosis; retrospective studies.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Mortality and loss to follow-up among HIV-infected persons on long-term antiretroviral therapy in Latin America and the Caribbean.J Int AIDS Soc. 2015 Jul 10;18(1):20016. doi: 10.7448/IAS.18.1.20016. eCollection 2015. J Int AIDS Soc. 2015. PMID: 26165322 Free PMC article.
-
Late presentation for HIV care in Southwest Ethiopia in 2003-2015: prevalence, trend, outcomes and risk factors.BMC Infect Dis. 2018 Jan 30;18(1):59. doi: 10.1186/s12879-018-2971-6. BMC Infect Dis. 2018. PMID: 29378523 Free PMC article.
-
Clinical outcomes of patients infected with HIV through use of injected drugs compared to patients infected through sexual transmission: late presentation, delayed anti-retroviral treatment and higher mortality.Addiction. 2016 Jul;111(7):1235-45. doi: 10.1111/add.13348. Epub 2016 Apr 14. Addiction. 2016. PMID: 26890155
-
Antiretroviral treatment regardless of CD4 count: the universal answer to a contextual question.AIDS Res Ther. 2016 Jul 26;13:27. doi: 10.1186/s12981-016-0111-1. eCollection 2016. AIDS Res Ther. 2016. PMID: 27462361 Free PMC article. Review.
-
The HIV care continuum in Latin America: challenges and opportunities.Lancet Infect Dis. 2015 Jul;15(7):833-9. doi: 10.1016/S1473-3099(15)00108-5. Lancet Infect Dis. 2015. PMID: 26122456 Review.
Cited by
-
Effect of AIDS-defining events at initiation of antiretroviral therapy on long-term mortality of HIV/AIDS patients in Southwestern China: a retrospective cohort study.AIDS Res Ther. 2020 Jul 17;17(1):44. doi: 10.1186/s12981-020-00300-4. AIDS Res Ther. 2020. PMID: 32680536 Free PMC article.
-
Pathways to Poor Adherence to Antiretroviral Therapy Among People Living with HIV: The Role of Food Insecurity and Alcohol Misuse.AIDS Behav. 2024 Apr;28(4):1173-1185. doi: 10.1007/s10461-023-04141-w. Epub 2023 Jul 31. AIDS Behav. 2024. PMID: 37523050
-
Microfluidic Devices for HIV Diagnosis and Monitoring at Point-of-Care (POC) Settings.Biosensors (Basel). 2022 Nov 1;12(11):949. doi: 10.3390/bios12110949. Biosensors (Basel). 2022. PMID: 36354458 Free PMC article. Review.
-
The HIV epidemic in Latin America: a time to reflect on the history of success and the challenges ahead.J Int AIDS Soc. 2020 Mar;23(3):e25468. doi: 10.1002/jia2.25468. J Int AIDS Soc. 2020. PMID: 32115884 Free PMC article. Review. No abstract available.
-
Early Antiretroviral Therapy in AIDS Patients Presenting With Toxoplasma gondii Encephalitis Is Associated With More Sequelae but Not Increased Mortality.Front Med (Lausanne). 2022 Feb 25;9:759091. doi: 10.3389/fmed.2022.759091. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35280886 Free PMC article.
References
-
- Joint United Nations Programme on HIV/AIDS AIDSinfo global AIDS monitoring database. http://www.aidsinfoonline.org/devinfo/libraries/aspx/dataview.aspx. Accessed August 15, 2017.
-
- Hernández-Ávila JE, Palacio-Mejía LS, Hernández-Romieu A, et al.. Effect of universal access to antiretroviral therapy on HIV/AIDS mortality in Mexico 1990–2011. J Acquir Immune Defic Syndr. 2015;69(3):e100–e108. - PubMed
-
- Joint United Nations Programme on HIV/AIDS The Gap report 2014. http://www.unaids.org/en/resources/campaigns/2014/2014gapreport/slides/. Accessed August 15, 2017.
-
- Ministerio de Salud y Desarrollo Social Boletín epidemiológico sobre VIH, sida e ITS en la Argentina, no. 31, año XXII, diciembre de 2019. http://www.msal.gob.ar/images/stories/bes/graficos/0000001754cnt-boletin.... Accessed October 9, 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
