

Babies in occiput posterior position are significantly more likely to require an emergency cesarean birth compared with babies in occiput transverse position in the second stage of labor: A prospective observational study
- PMID: 31667835
- PMCID: PMC7154761
- DOI: 10.1111/aogs.13765
Babies in occiput posterior position are significantly more likely to require an emergency cesarean birth compared with babies in occiput transverse position in the second stage of labor: A prospective observational study
Abstract
Introduction: Malposition complicates 2-13% of births at delivery, leading to increased obstetric interventions (cesarean section and instrumental delivery) and higher rates of adverse fetal and maternal outcomes. Limited data are available regarding the likely rates of obstetric intervention and subsequent neonatal and maternal outcomes of births with babies in persistent occiput posterior position vs those in persistent occiput transverse position. The UK Audit and Research trainee Collaborative in Obstetrics and Gynecology (UK-ARCOG) network set out to collect data prospectively at delivery on final mode of delivery and immediate outcomes.
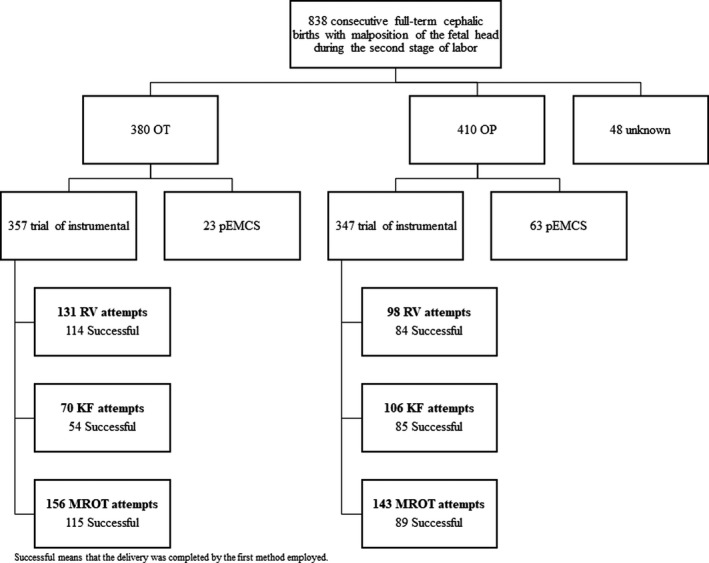
Material and methods: The UK-ARCOG network collected data on all births with malposition of the fetal head complicating the second stage of labor (n = 838) (occiput posterior/occiput transverse) requiring rotational vaginal operative birth or emergency cesarean to expedite delivery across 66 participating UK National Health Service maternity units over a 1-month period. The outcomes considered were the need for emergency cesarean section without a trial of instrumental delivery, success of the first method of delivery employed in achieving a vaginal delivery and neonatal/maternal outcomes.
Results: Obstetricians regarded assistance with an operative vaginal delivery method to be unsafe in 15% of babies in occiput posterior position and 6.1% of babies in occiput transverse position, and they were delivered by primary emergency cesarean section. When vaginal delivery was deemed safe (defined as attempted assisted vaginal rotational delivery), the first instrument attempted was successful in 74.4% of occiput posterior babies and 79.3% of occiput transverse babies.
Conclusions: Our data facilitates decision making by obstetricians to increase safety of assisted rotational operative delivery of a malpositioned baby at initial assessment and in counseling women. Until data from a well-designed randomized controlled trial of instrumental delivery vs emergency cesarean section are available, this manuscript provides contemporaneous national data from a high resource setting within a structured training program, to assist the selection of an appropriate instrument/method for the delivery of a malpositioned baby.
Keywords: Kielland forceps; cesarean section; manual rotation; occiput posterior; occiput transverse; rotational delivery; rotational ventouse.
© 2019 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Caughey AB, Sharshiner R, Cheng YW. Fetal malposition: impact and management. Clin Obstet Gynecol. 2015;58:241‐245. - PubMed
-
- Le Ray C, Serres P, Schmitz T, Cabrol D, Goffinet F. Manual rotation in occiput posterior or transverse positions: risk factors and consequences on the cesarean delivery rate. Obstet Gynecol. 2007;110:873‐879. - PubMed
-
- Shaffer BL, Cheng YW, Vargas JE, Caughey AB. Manual rotation to reduce caesarean delivery in persistent occiput posterior or transverse position. J Matern Fetal Neonatal Med. 2011;24:65‐72. - PubMed
-
- Tempest N, Hart A, Walkinshaw S, Hapangama DK. A re‐evaluation of the role of rotational forceps: retrospective comparison of maternal and perinatal outcomes following different methods of birth for malposition in the second stage of labour. BJOG. 2013;120:1277‐1284. - PubMed
