

Evidence-based clinical practice guideline on antibiotic use for the urgent management of pulpal- and periapical-related dental pain and intraoral swelling: A report from the American Dental Association
- PMID: 31668170
- PMCID: PMC8270006
- DOI: 10.1016/j.adaj.2019.08.020
Evidence-based clinical practice guideline on antibiotic use for the urgent management of pulpal- and periapical-related dental pain and intraoral swelling: A report from the American Dental Association
Abstract
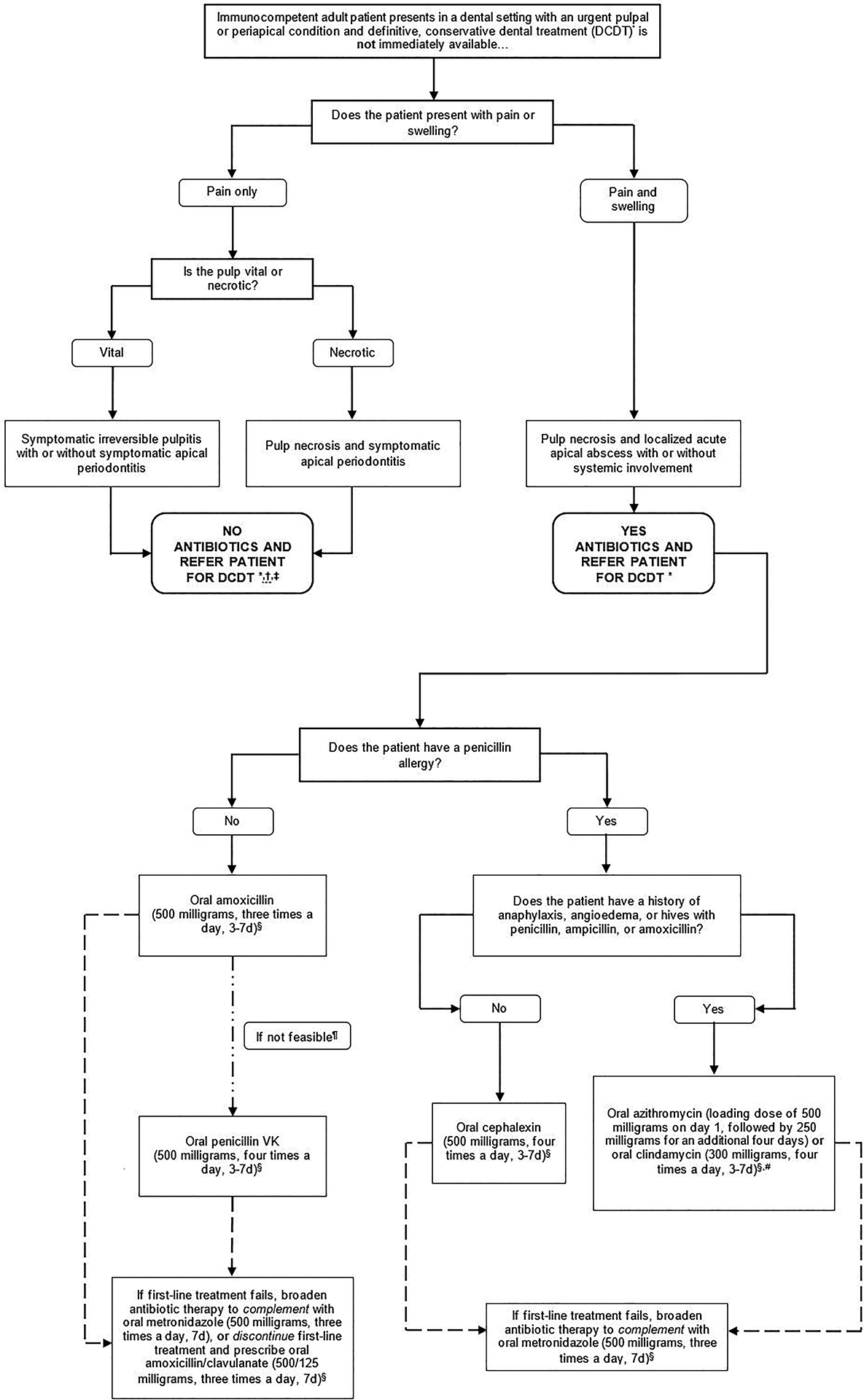
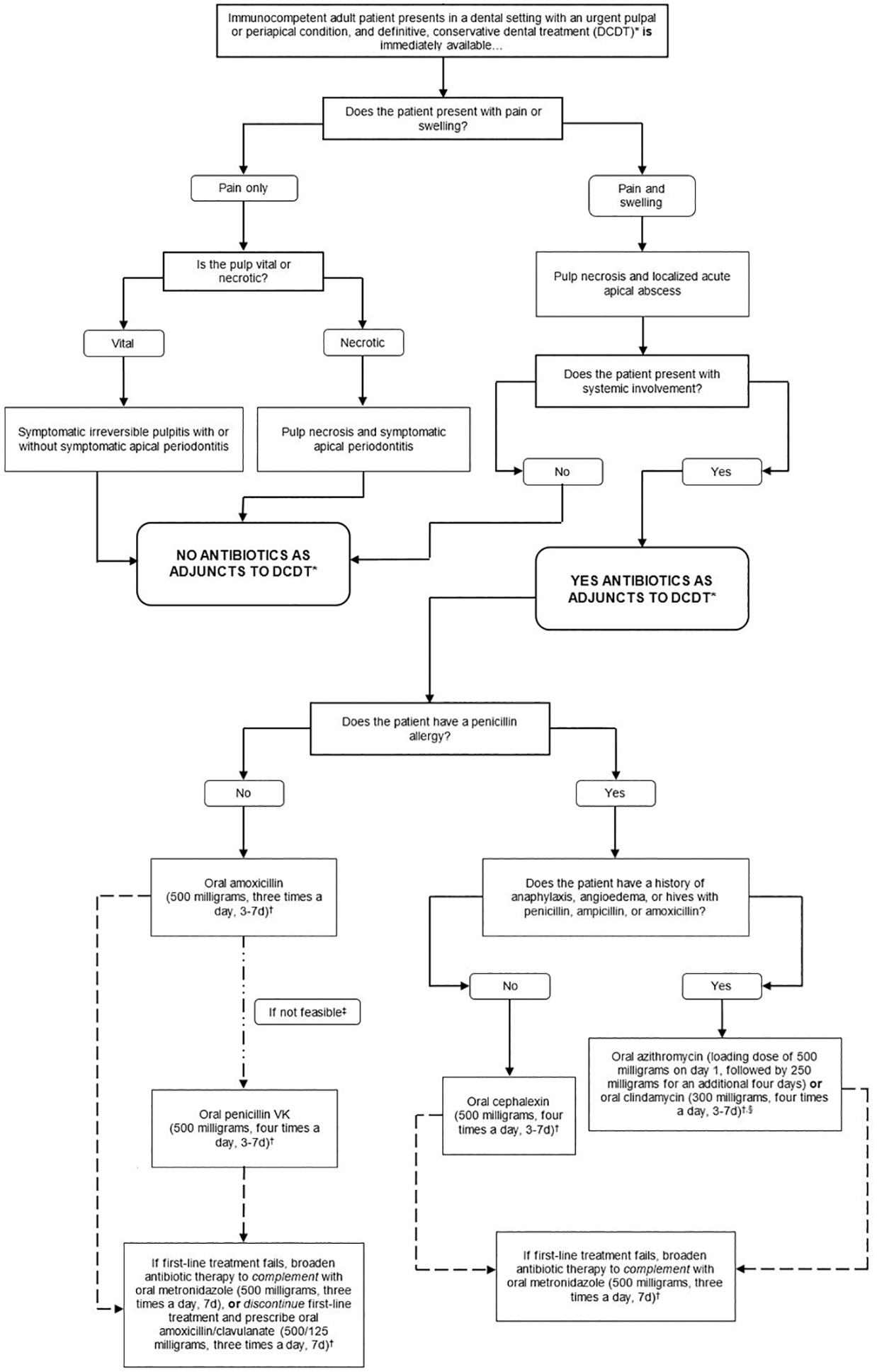
Background: An expert panel convened by the American Dental Association Council on Scientific Affairs and the Center for Evidence-Based Dentistry conducted a systematic review and formulated clinical recommendations for the urgent management of symptomatic irreversible pulpitis with or without symptomatic apical periodontitis, pulp necrosis and symptomatic apical periodontitis, or pulp necrosis and localized acute apical abscess using antibiotics, either alone or as adjuncts to definitive, conservative dental treatment (DCDT) in immunocompetent adults.
Types of studies reviewed: The authors conducted a search of the literature in MEDLINE, Embase, the Cochrane Library, and the Cumulative Index to Nursing and Allied Health Literature to retrieve evidence on benefits and harms associated with antibiotic use. The authors used the Grading of Recommendations Assessment, Development and Evaluation approach to assess the certainty in the evidence and the Evidence-to-Decision framework.
Results: The panel formulated 5 clinical recommendations and 2 good practice statements, each specific to the target conditions, for settings in which DCDT is and is not immediately available. With likely negligible benefits and potentially large harms, the panel recommended against using antibiotics in most clinical scenarios, irrespective of DCDT availability. They recommended antibiotics in patients with systemic involvement (for example, malaise or fever) due to the dental conditions or when the risk of experiencing progression to systemic involvement is high.
Conclusion and practical implications: Evidence suggests that antibiotics for the target conditions may provide negligible benefits and probably contribute to large harms. The expert panel suggests that antibiotics for target conditions be used only when systemic involvement is present and that immediate DCDT should be prioritized in all cases.
Keywords: Antibiotics; antibiotic stewardship; clinical practice guideline; localized acute apical abscess; pulp necrosis; symptomatic apical periodontitis; symptomatic irreversible pulpitis.
Copyright © 2019 American Dental Association. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Cohen LA, Bonito AJ, Akin DR, et al. Toothache pain: a comparison of visits to physicians, emergency departments and dentists. J Am Dent Assoc 2008;139(9):1205–16. - PubMed
-
- Kelekar U, Naavaal S. Dental visits and associated emergency department-charges in the United States: Nationwide Emergency Department Sample, 2014. J Am Dent Assoc 2019;150(4):305–12 e1. - PubMed
-
- Shah AC, Leong KK, Lee MK, Allareddy V. Outcomes of hospitalizations attributed to periapical abscess from 2000 to 2008: a longitudinal trend analysis. J Endod 2013;39(9):1104–10. - PubMed
-
- Glossary of Endodontic Terms. American Association of Endodontists: American Association of Endodontists 2015. “http://www.nxtbook.com/nxtbooks/aae/endodonticglossary2016/index.php“. Accessed December 10 2018.
Appendix References
-
- Appropriate Use Criteria For the Management of Patients with Orthopaedic Implants Undergoing Dental Procedures. American Academy of Orthopaedic Surgeons 2016. “https://www.aaos.org/uploadedFiles/PreProduction/Quality/AUCs_and_Perfor...“. - PubMed
-
- Acquired Immunodeficiency Syndrome (AIDS). U.S Department of Health and Human Services 2018. “https://aidsinfo.nih.gov/contentfiles/glossaryhivrelatedterms_english.pdf“. Accessed May 25 2019.
-
- Revised Surveillance Case Definition for HIV Infection - United States, 2014. Centers for Disease Control and Prevention 2014. “https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6303a1.htm“. Accessed May 25 2019.
-
- Brooks L, Shaw A, Sharp D, Hay AD. Towards a better understanding of patients’ perspectives of antibiotic resistance and MRSA: a qualitative study. Fam Pract 2008;25(5):341–8. - PubMed
-
- Wagstaff B. Impact of antibiotic restrictions: the patient’s perspective. Clin Microbiol Infect 2006;12 Suppl 5:10–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
