

Radioembolization Plus Chemotherapy for First-line Treatment of Locally Advanced Intrahepatic Cholangiocarcinoma: A Phase 2 Clinical Trial
- PMID: 31670746
- PMCID: PMC6824230
- DOI: 10.1001/jamaoncol.2019.3702
Radioembolization Plus Chemotherapy for First-line Treatment of Locally Advanced Intrahepatic Cholangiocarcinoma: A Phase 2 Clinical Trial
Abstract
Importance: Patients with unresectable intrahepatic cholangiocarcinoma (ICC) have a poor prognosis. Selective internal radiotherapy (SIRT) is a promising treatment option for hepatic tumors, but no prospective studies of combination SIRT with chemotherapy have been published to our knowledge.
Objective: To determine the response rate after SIRT combined with chemotherapy in patients with unresectable ICC.
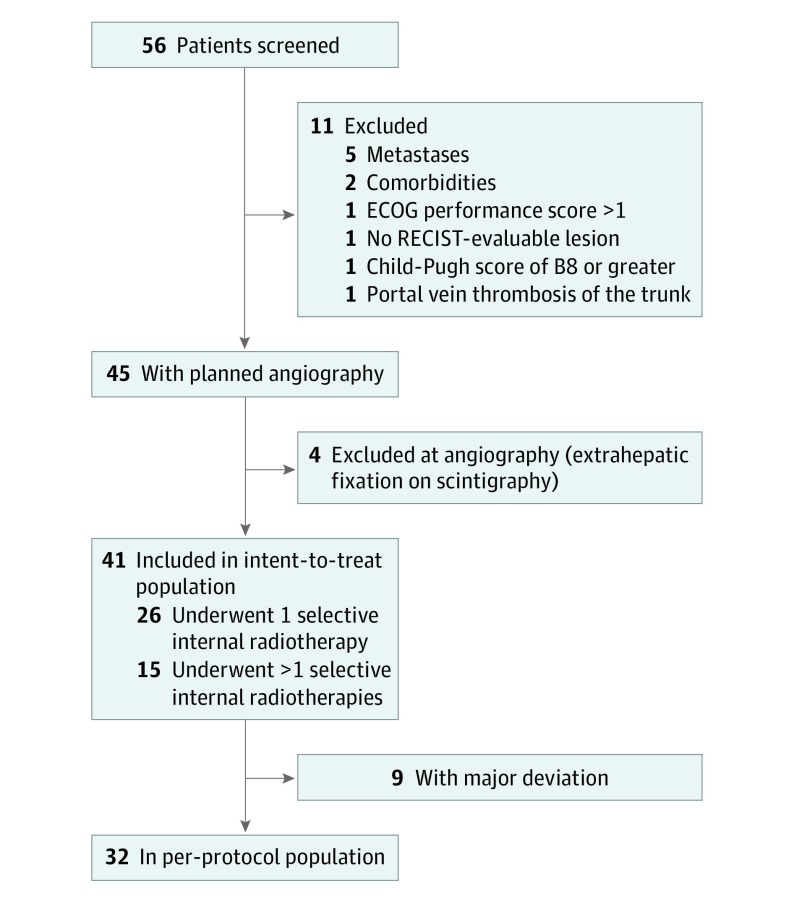
Design, setting, and participants: This phase 2 clinical trial, the Yttrium-90 Microspheres in Cholangiocarcinoma (MISPHEC) trial, included patients with unresectable ICC who have never received chemotherapy or intra-arterial therapy and were treated at 7 centers which had experience with SIRT between November 12, 2013, and June 21, 2016. Statistical analysis was performed from March 31, 2017, to June 17, 2019.
Interventions: Concomitant first-line chemotherapy with cisplatin, 25 mg/m2, and gemcitabine, 1000 mg/m2 (gemcitabine reduced to 300 mg/m2 for the cycles just before and after SIRT), on days 1 and 8 of a 21-day cycle for 8 cycles. Selective internal radiotherapy was administered during cycle 1 (1 hemiliver disease) or cycles 1 and 3 (disease involving both hemilivers) using glass Y90 microspheres.
Main outcomes and measures: Response rate at 3 months according to Response Evaluation Criteria in Solid Tumors (RECIST) 1.1. Secondary end points were toxic effects, progression-free survival, overall survival, disease control rate, and response rate according to Choi criteria.
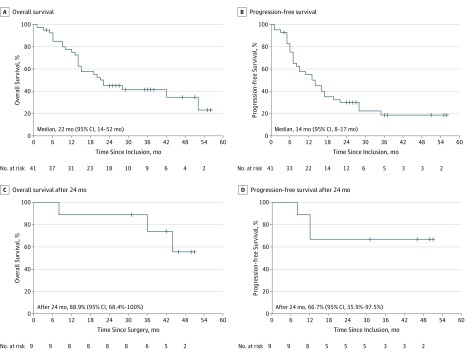
Results: Of 41 patients included in the study, 26 (63%) were male, with a mean (SD) age of 64.0 (10.7) years. Response rate according to RECIST was 39% (90% CI, 26%-53%) at 3 months according to local review and was confirmed at 41% as best response by central review; disease control rate was 98%. According to Choi criteria, the response rate was 93%. After a median follow-up of 36 months (95% CI, 26-52 months), median progression-free survival was 14 months (95% CI, 8-17 months), with progression-free survival rates of 55% at 12 months and 30% at 24 months. Median overall survival was 22 months (95% CI, 14-52 months), with overall survival rates of 75% at 12 months and 45% at 24 months. Of 41 patients, 29 (71%) had grades 3 to 4 toxic effects; 9 patients (22%) could be downstaged to surgical intervention, with 8 (20%) achieving R0 (microscopic-free margins) surgical resection. After a median of 46 months (95% CI, 31 months to not reached) after surgery, median relapse-free survival was not reached among patients who underwent resection.
Conclusions and relevance: Combination chemotherapy and SIRT had antitumor activity as first-line treatment of unresectable ICC, and a significant proportion of patients were downstaged to surgical intervention. A phase 3 trial is ongoing.
Conflict of interest statement
Figures

Comment in
-
Moving the Needle Forward With Locoregional Treatment in Unresectable Cholangiocarcinoma-The Jury Is Still Out.JAMA Oncol. 2020 Jan 1;6(1):29-31. doi: 10.1001/jamaoncol.2019.3691. JAMA Oncol. 2020. PMID: 31670748 No abstract available.
-
About the Recently Published Paper on JAMA Oncology "Radioembolization Plus Chemotherapy for First-Line Treatment of Locally Advanced Intrahepatic Cholangiocarcinoma: A Phase 2 Clinical Trial".Cardiovasc Intervent Radiol. 2020 Sep;43(9):1418-1419. doi: 10.1007/s00270-020-02577-4. Epub 2020 Jul 16. Cardiovasc Intervent Radiol. 2020. PMID: 32676960 No abstract available.
