

Follow-up ultrasound in second-trimester low-positioned anterior and posterior placentae: prospective cohort study
- PMID: 31671480
- PMCID: PMC7702149
- DOI: 10.1002/uog.21903
Follow-up ultrasound in second-trimester low-positioned anterior and posterior placentae: prospective cohort study
Erratum in
-
Corrigendum.Ultrasound Obstet Gynecol. 2020 Dec;56(6):967. doi: 10.1002/uog.23547. Ultrasound Obstet Gynecol. 2020. PMID: 33259101 Free PMC article. No abstract available.
Abstract
Objectives: The majority of cases of placenta previa or a low-lying placenta in the second trimester will have a normal placental position in the third trimester. The aim of this study was to assess the accuracy of the distance between the placenta and the internal os of the cervix (IOD) in the second trimester for the prediction of third-trimester low-positioned placenta, and to define a cut-off value at which all cases of third-trimester low-positioned placenta are identified.
Methods: This was a prospective cohort study including women undergoing a transvaginal ultrasound examination between 18 and 24 weeks' gestation who had a low-positioned placenta, defined as an IOD of < 20 mm. Low-positioned placenta included placenta previa, defined as a placenta covering the internal os of the cervix, and a low-lying placenta, defined as a placenta lying near to (within 20 mm) but not overlying the internal os. All women were re-evaluated in the third trimester. Relative risks for a low-positioned placenta in the third trimester were calculated for women with placenta previa vs a low-lying placenta, posterior vs anterior placenta and positive vs negative history of Cesarean section. Multilevel likelihood ratios for ranges of IOD in the prediction of a low-positioned placenta in the third trimester were calculated separately for anteriorly and posteriorly located placentae. Corresponding receiver-operating-characteristics curves were constructed.
Results: In total, 958 women were included in the study. In the second trimester, placentae were more frequently located on the posterior side (62.0%) than on the anterior side (38.0%). In the third trimester, 48/958 (5.0%) placentae persisted as a low-positioned placenta. Women with placenta previa in the second trimester had a higher risk of a low-positioned placenta in the third trimester than did those with a low-lying placenta in the second trimester (37/181 (20.4%) vs 11/777 (1.4%); relative risk (RR), 17.9 (95% CI, 8.9-36.0)). Women with a posterior placenta had a higher risk of a low-positioned placenta in the third trimester than did those with an anterior placenta (38/594 (6.4%) vs 10/364 (2.7%); RR, 2.4 (95% CI, 1.2-4.9)), as did women with a history of Cesarean section compared with those without such a history (14/105 (13.3%) vs 34/853 (4.0%); RR, 3.7 (95% CI, 1.9-7.2)). The cut-off value of IOD in the second trimester to identify all cases of an abnormally located placenta in the third trimester was 15.5 mm for posteriorly located placentae, while for anteriorly located placentae the IOD cut-off was lower, namely -4.5 mm, representing a 4.5-mm overlap of the placental edge over the internal os of the cervix.
Conclusions: With incorporation of a safety margin of 5 mm and ensuring that all women with placenta previa undergo a follow-up scan, we recommend lowering the IOD cut-off value for follow-up in cases of an anterior low-positioned placenta from 20 to 5 mm, which would decrease the number of unnecessary follow-up ultrasound examinations without missing any high-risk women. © 2019 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of International Society of Ultrasound in Obstetrics and Gynecology.
Keywords: low-lying placenta; migration; placenta previa; second trimester; ultrasonography.
© 2019 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of International Society of Ultrasound in Obstetrics and Gynecology.
Figures
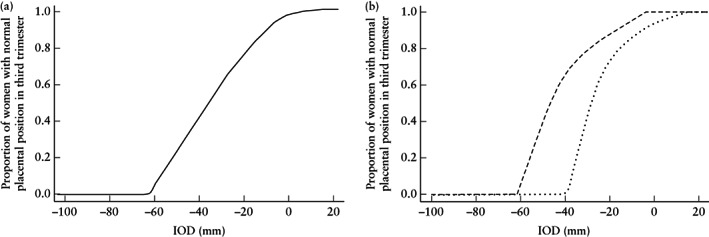
 ) or posterior (
) or posterior ( ) placenta (b).
) placenta (b).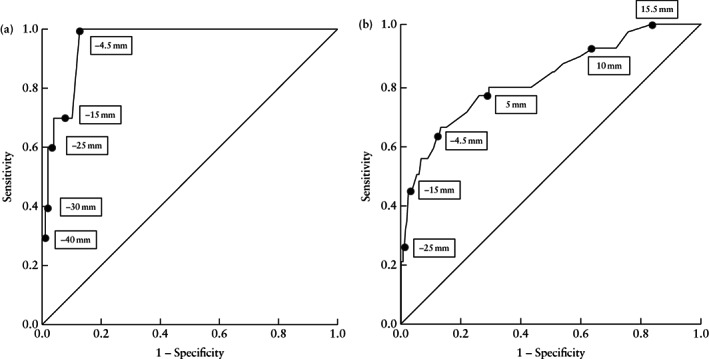
References
-
- Crane JM, Van den Hof MC, Dodds L, Armson BA, Liston R. Maternal complications with placenta previa. Am J Perinatol 2000; 17: 101–105. - PubMed
-
- Iyasu S, Saftlas AK, Rowley DL, Koonin LM, Lawson HW, Atrash HK. The epidemiology of placenta previa in the United States, 1979 through 1987. Am J Obstet Gynecol 1993; 168: 1424–1429. - PubMed
-
- Ananth CV, Demissie K, Smulian JC, Vintzileos AM. Placenta previa in singleton and twin births in the United States, 1989 through 1998: a comparison of risk factor profiles and associated conditions. Am J Obstet Gynecol 2003; 188: 275–281. - PubMed
-
- Ruiter L, Kok N, Limpens J, Derks JB, de Graaf IM, Mol B, Pajkrt E. Incidence of and risk indicators for vasa praevia: a systematic review. BJOG 2016; 123: 1278–1287. - PubMed
-
- Reddy UM, Abuhamad AZ, Levine D, Saade GR; Fetal Imaging Workshop Invited Participants. Fetal imaging: executive summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal–Fetal Medicine, American Institute of Ultrasound in Medicine, American College of Obstetricians and Gynecologists, American College of Radiology, Society for Pediatric Radiology, and Society of Radiologists in Ultrasound Fetal Imaging workshop. Obstet Gynecol 2014; 123: 1070–1082. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
