

ST-Segment-Elevation Myocardial Infarction (STEMI) Patients Without Standard Modifiable Cardiovascular Risk Factors-How Common Are They, and What Are Their Outcomes?
- PMID: 31672080
- PMCID: PMC6898813
- DOI: 10.1161/JAHA.119.013296
ST-Segment-Elevation Myocardial Infarction (STEMI) Patients Without Standard Modifiable Cardiovascular Risk Factors-How Common Are They, and What Are Their Outcomes?
Abstract
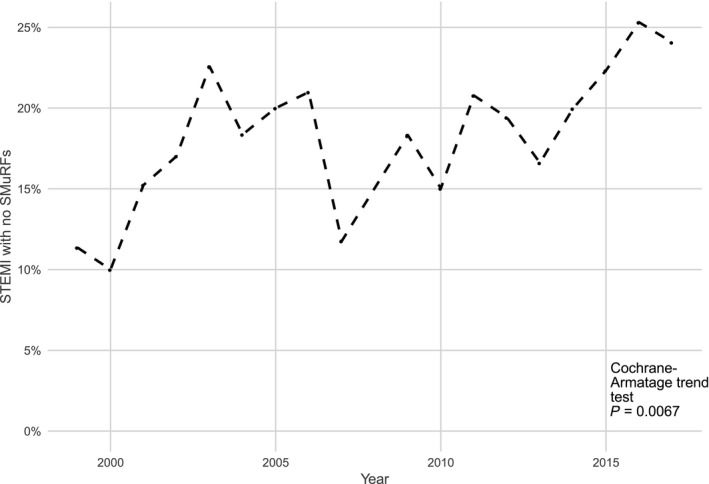
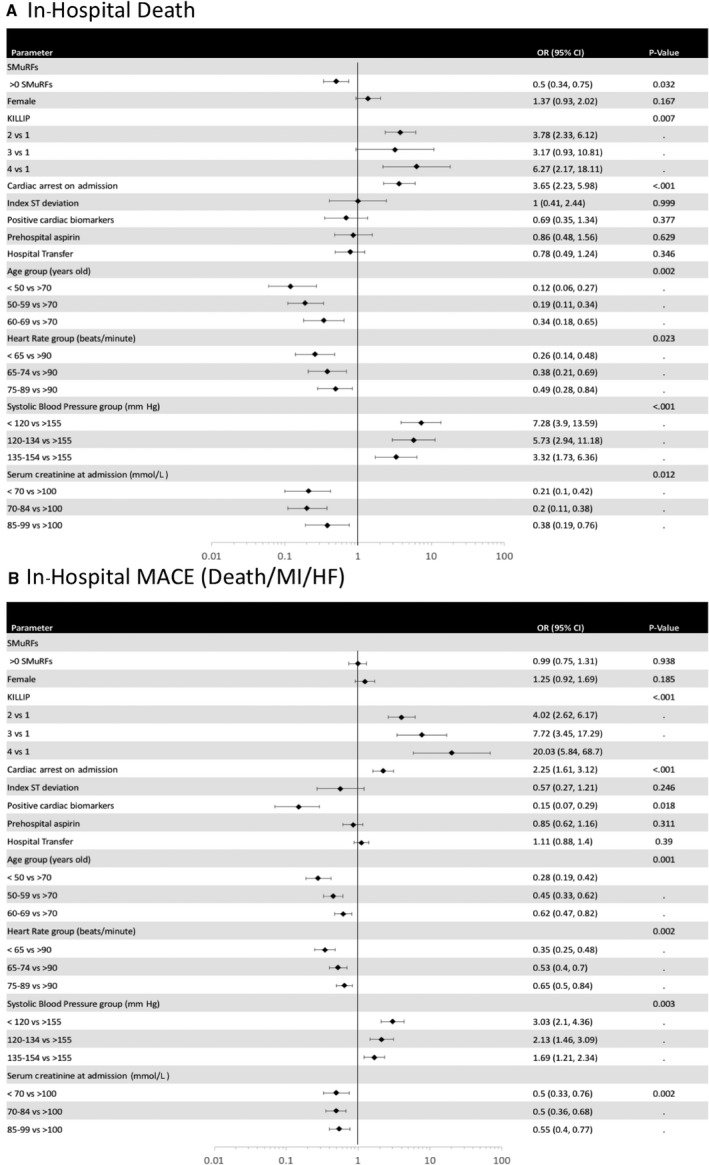
Background Programs targeting the standard modifiable cardiovascular risk factors (SMuRFs: hypertension, diabetes mellitus, hypercholesterolemia, smoking) are critical to tackling coronary heart disease at a community level. However, myocardial infarction in SMuRF-less individuals is not uncommon. This study uses 2 sequential large, multicenter registries to examine the proportion and outcomes of SMuRF-less ST-segment-elevation myocardial infarction (STEMI) patients. Methods and Results We identified 3081 STEMI patients without a prior history of cardiovascular disease in the Australian GRACE (Global Registry of Acute Coronary Events) and CONCORDANCE (Cooperative National Registry of Acute Coronary Syndrome Care) registries, encompassing 42 hospitals, between 1999 and 2017. We examined the proportion that were SMuRF-less as well as outcomes. The primary outcome was in-hospital mortality, and the secondary outcome was major adverse cardiovascular events (death, myocardial infarction, or heart failure, during the index admission). Multivariate regression models were used to identify predictors of major adverse cardiovascular events. Of STEMI patients without a prior history of cardiovascular disease 19% also had no history of SMuRFs. This proportion increased from 14% to 23% during the study period (P=0.0067). SMuRF-less individuals had a higher in-hospital mortality rate than individuals with 1 or more SMuRFs. There were no clinically significant differences in major adverse cardiovascular events at 6 months between the 2 groups. Conclusions A substantial and increasing proportion of STEMI presentations occur independently of SMuRFs. Discovery of new markers and mechanisms of disease beyond standard risk factors may facilitate novel preventative strategies. Studies to assess longer-term outcomes of SMuRF-less STEMI patients are warranted.
Keywords: ST‐segment–elevation myocardial infarction; atherosclerosis; mortality; risk factor.
Figures
References
-
- Kannel WB, Dawber TR, Kagan A, Revotskie N, Stokes J III. Factors of risk in the development of coronary heart disease—six year follow‐up experience. The Framingham Study. Ann Intern Med. 1961;55:33–50. - PubMed
-
- Wilson PW, D'Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998;97:1837–1847. - PubMed
-
- Ridker PM, Buring JE, Rifai N, Cook NR. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: the Reynolds Risk Score. JAMA. 2007;297:611–619. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
