

Association of statin use and clinical outcomes in heart failure patients: a systematic review and meta-analysis
- PMID: 31672151
- PMCID: PMC6822388
- DOI: 10.1186/s12944-019-1135-z
Association of statin use and clinical outcomes in heart failure patients: a systematic review and meta-analysis
Erratum in
-
Correction to: Association of statin use and clinical outcomes in heart failure patients: a systematic review and meta-analysis.Lipids Health Dis. 2020 Sep 20;19(1):208. doi: 10.1186/s12944-020-01380-x. Lipids Health Dis. 2020. PMID: 32951597 Free PMC article.
Abstract
Background: The role of statins in patients with heart failure (HF) of different levels of left ventricular ejection fraction (LVEF) remains unclear especially in the light of the absence of prospective data from randomized controlled trials (RCTs) in non-ischemic HF, and taking into account potential statins' prosarcopenic effects. We assessed the association of statin use with clinical outcomes in patients with HF.
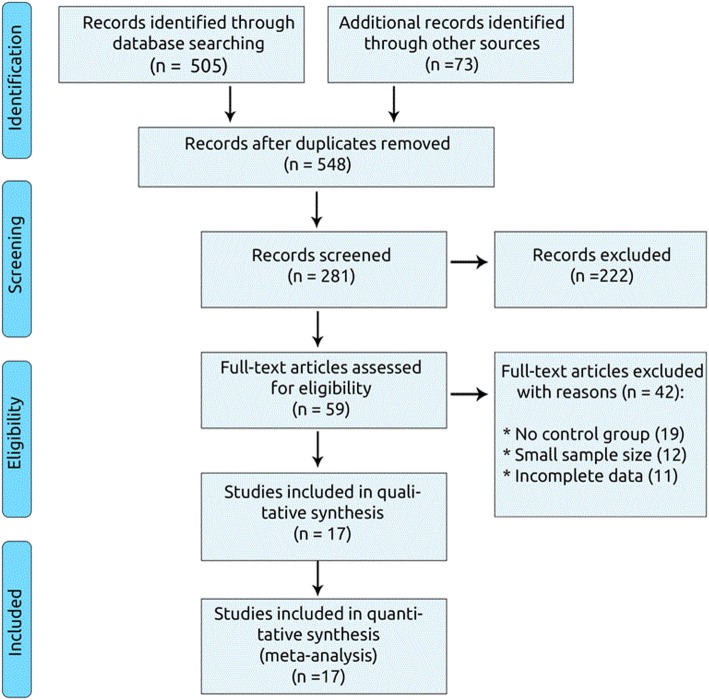
Methods: We searched PubMed, EMBASE, Scopus, Google Scholar and Cochrane Central until August 2018 for RCTs and prospective cohorts comparing clinical outcomes with statin vs non-statin use in patients with HF at different LVEF levels. We followed the guidelines of the 2009 PRISMA statement for reporting and applied independent extraction by multiple observers. Meta-analyses of hazard ratios (HRs) of effects of statins on clinical outcomes used generic inverse variance method and random model effects. Clinical outcomes were all-cause mortality, cardiovascular (CV) mortality and CV hospitalization.
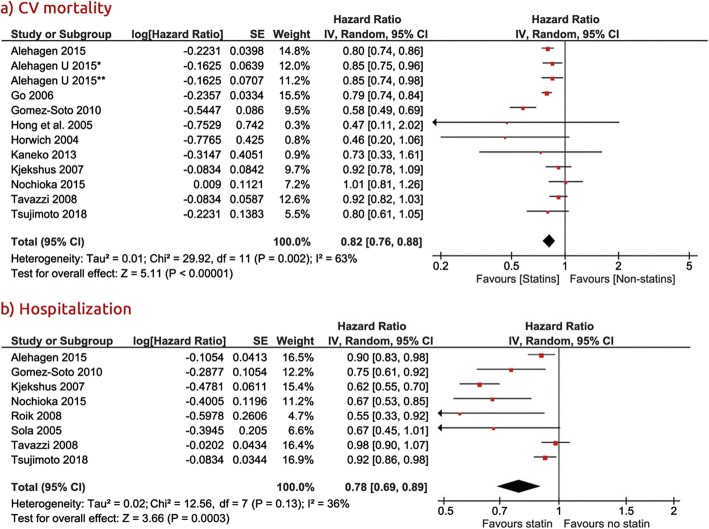
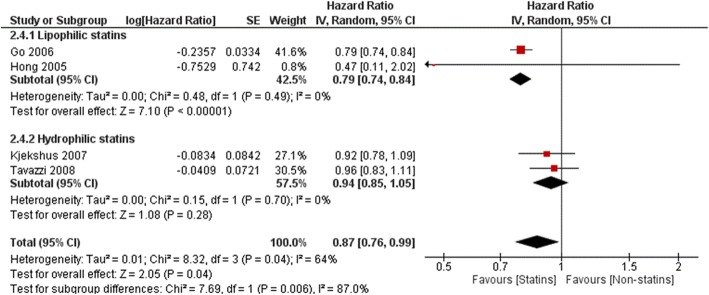
Results: Finally we included 17 studies (n = 88,100; 2 RCTs and 15 cohorts) comparing statin vs non-statin users (mean follow-up 36 months). Compared with non-statin use, statin use was associated with lower risk of all-cause mortality (HR 0.77, 95% confidence interval [CI], 0.72-0.83, P < 0.0001, I2 = 63%), CV mortality (HR 0.82, 95% CI: 0.76-0.88, P < 0.0001, I2 = 63%), and CV hospitalization (HR 0.78, 95% CI: 0.69-0.89, P = 0.0003, I2 = 36%). All-cause mortality was reduced on statin therapy in HF with both EF < 40% and ≥ 40% (HR: 0.77, 95% Cl: 0.68-0.86, P < 0.00001, and HR 0.75, 95% CI: 0.69-0.82, P < 0.00001, respectively). Similarly, CV mortality (HR 0.86, 95% CI: 0.79-0.93, P = 0.0003, and HR 0.83, 95% CI: 0.77-0.90, P < 0.00001, respectively), and CV hospitalizations (HR 0.80 95% CI: 0.64-0.99, P = 0.04 and HR 0.76 95% CI: 0.61-0.93, P = 0.009, respectively) were reduced in these EF subgroups. Significant effects on all clinical outcomes were also found in cohort studies' analyses; the effect was also larger and significant for lipophilic than hydrophilic statins.
Conclusions: In conclusion, statins may have a beneficial effect on CV outcomes irrespective of HF etiology and LVEF level. Lipophilic statins seem to be much more favorable for patients with heart failure.
Keywords: Heart failure; Hospitalization; Meta-analysis; Mortality; Statins.
Conflict of interest statement
ABD, IB, JR, JJ, SvH, and AVH have no conflicts of interest to disclose; DPM has given talks and attended conferences sponsored by MSD, AstraZeneca and Libytec; SDA reports personal fees from Bayer, Boehringer Ingelheim, Vifor, Servier and Novartis, outside the submitted work; MB has served on the speakers bureau of Abbott/Mylan, Abbott Vascular, Actavis, Akcea, Amgen, Biofarm, KRKA, MSD, Sanofi-Aventis, Servier and Valeant, and has served as a consultant to Abbott Vascular, Akcea, Amgen, Daichii Sankyo, Esperion, Lilly, MSD, Resverlogix, Sanofi-Aventis; Grants from Sanofi and Valeant.
Figures






References
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. 2014;129:S1–45. doi: 10.1161/01.cir.0000437738.63853.7a. - DOI - PubMed
-
- Ponikowski P, Voors AA, Anker SD, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2016;37(27):2129–200. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
