

TFEB activation in macrophages attenuates postmyocardial infarction ventricular dysfunction independently of ATG5-mediated autophagy
- PMID: 31672943
- PMCID: PMC6948771
- DOI: 10.1172/jci.insight.127312
TFEB activation in macrophages attenuates postmyocardial infarction ventricular dysfunction independently of ATG5-mediated autophagy
Abstract
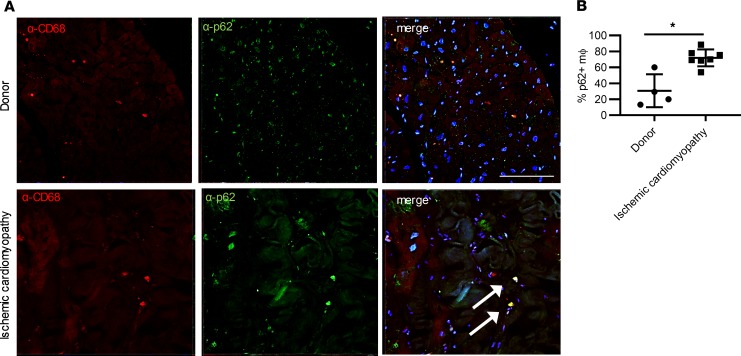
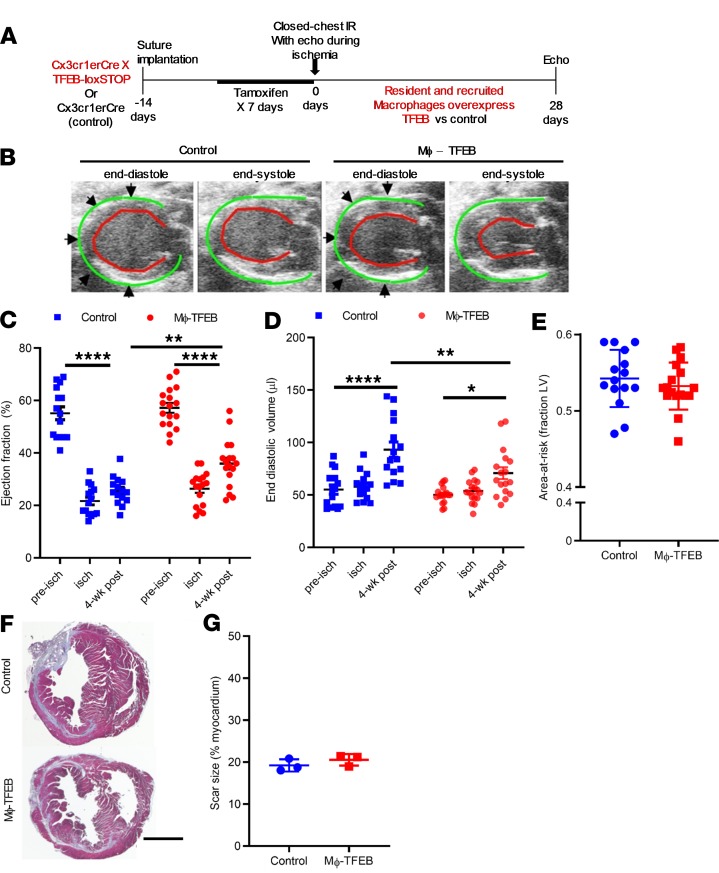
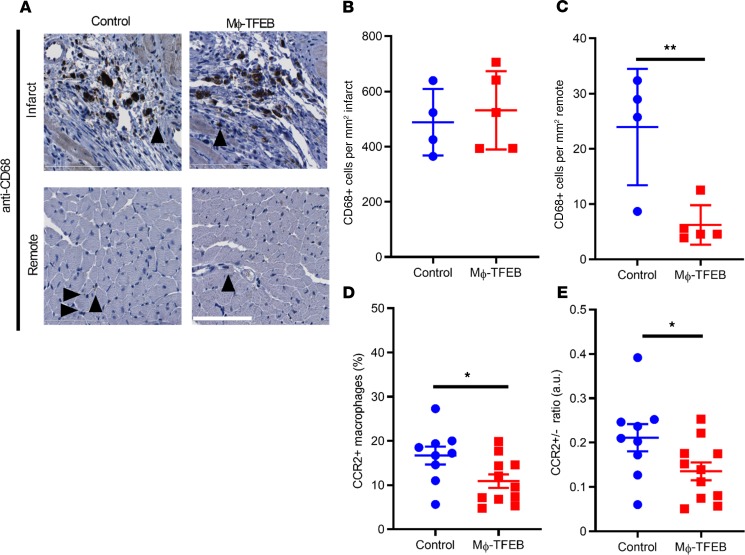
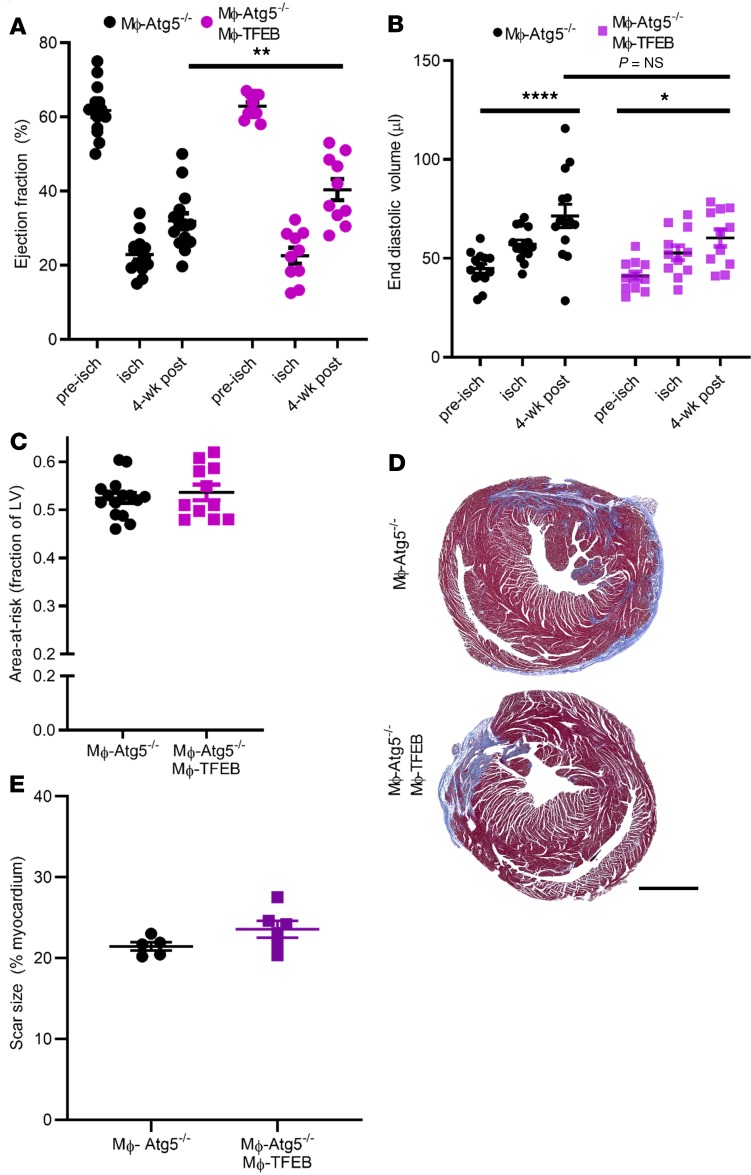
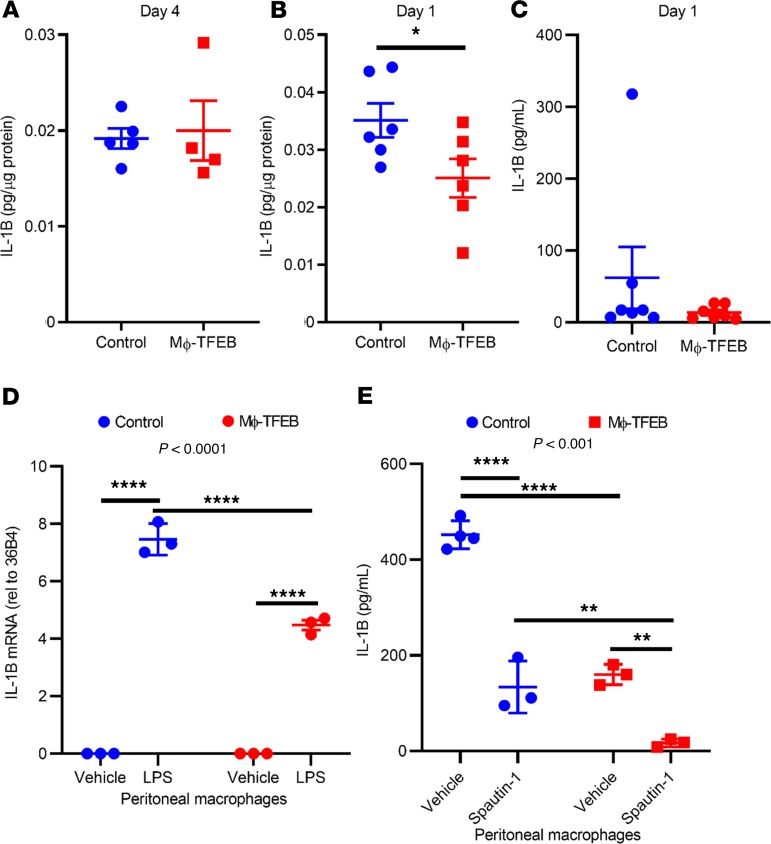
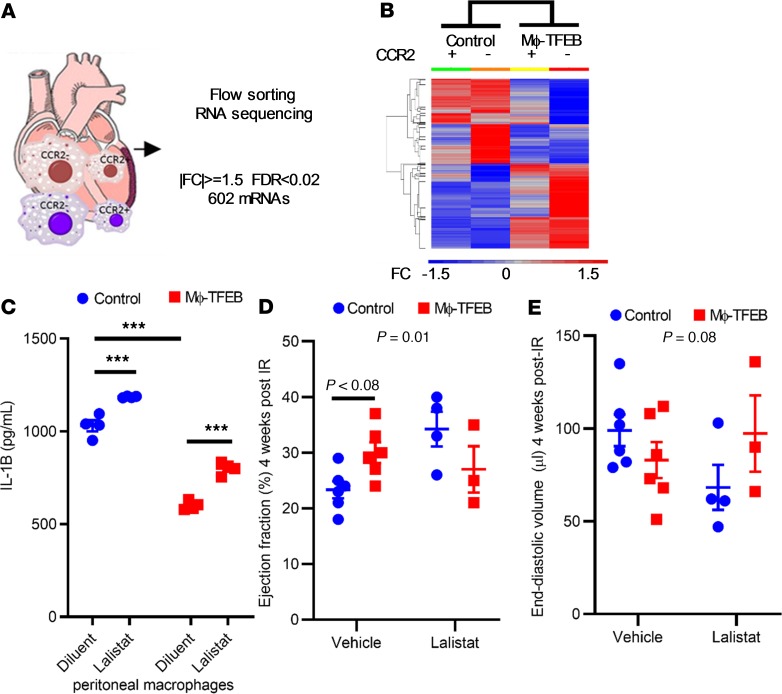
Lysosomes are at the epicenter of cellular processes critical for inflammasome activation in macrophages. Inflammasome activation and IL-1β secretion are implicated in myocardial infarction (MI) and resultant heart failure; however, little is known about how macrophage lysosomes regulate these processes. In mice subjected to cardiac ischemia/reperfusion (IR) injury and humans with ischemic cardiomyopathy, we observed evidence of lysosomal impairment in macrophages. Inducible macrophage-specific overexpression of transcription factor EB (TFEB), a master regulator of lysosome biogenesis (Mϕ-TFEB), attenuated postinfarction remodeling, decreased abundance of proinflammatory macrophages, and reduced levels of myocardial IL-1β compared with controls. Surprisingly, neither inflammasome suppression nor Mϕ-TFEB-mediated attenuation of postinfarction myocardial dysfunction required intact ATG5-dependent macroautophagy (hereafter termed "autophagy"). RNA-seq of flow-sorted macrophages postinfarction revealed that Mϕ-TFEB upregulated key targets involved in lysosomal lipid metabolism. Specifically, inhibition of the TFEB target, lysosomal acid lipase, in vivo abrogated the beneficial effect of Mϕ-TFEB on postinfarction ventricular function. Thus, TFEB reprograms macrophage lysosomal lipid metabolism to attenuate remodeling after IR, suggesting an alternative paradigm whereby lysosome function affects inflammation.
Keywords: Autophagy; Cardiology; Inflammation; Lysosomes; Macrophages.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL125838/HL/NHLBI NIH HHS/United States
- R01 HL143431/HL/NHLBI NIH HHS/United States
- R01 HL107594/HL/NHLBI NIH HHS/United States
- R01 NS094692/NS/NINDS NIH HHS/United States
- S10 RR027552/RR/NCRR NIH HHS/United States
- P30 DK056341/DK/NIDDK NIH HHS/United States
- T32 HL007081/HL/NHLBI NIH HHS/United States
- R01 DK110034/DK/NIDDK NIH HHS/United States
- R01 HL139714/HL/NHLBI NIH HHS/United States
- P30 DK052574/DK/NIDDK NIH HHS/United States
- I01 BX003415/BX/BLRD VA/United States
- R01 HL138466/HL/NHLBI NIH HHS/United States
- P30 DK020579/DK/NIDDK NIH HHS/United States
- K08 HL138262/HL/NHLBI NIH HHS/United States
- I01 BX004235/BX/BLRD VA/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
