

Prevalence and determinants of type 2 diabetes among lean African migrants and non-migrants: the RODAM study
- PMID: 31673340
- PMCID: PMC6815658
- DOI: 10.7189/jogh.09.020426
Prevalence and determinants of type 2 diabetes among lean African migrants and non-migrants: the RODAM study
Abstract
Background: Exposure to adverse conditions earlier in life-course can predispose to type 2 diabetes in adulthood, irrespective of body mass index (BMI). However, the burden of type 2 diabetes in lean Africans is not well understood despite higher exposure to adverse early life conditions. Mirroring ongoing epidemiological transition, we assessed the burden and determinants of type 2 diabetes in a homogenous group of lean Ghanaians residing in rural and urban Ghana, and as migrants in Europe.
Methods: Baseline data from 2179 RODAM study participants with BMI<25kg/m2 (25-70 years) were analyzed. Prevalence and determinants of type 2 diabetes were estimated using logistic regression analysis. Adjustments were made for socio-demographic and lifestyle factors, use of anti-diabetic medication and optimal blood glucose control.
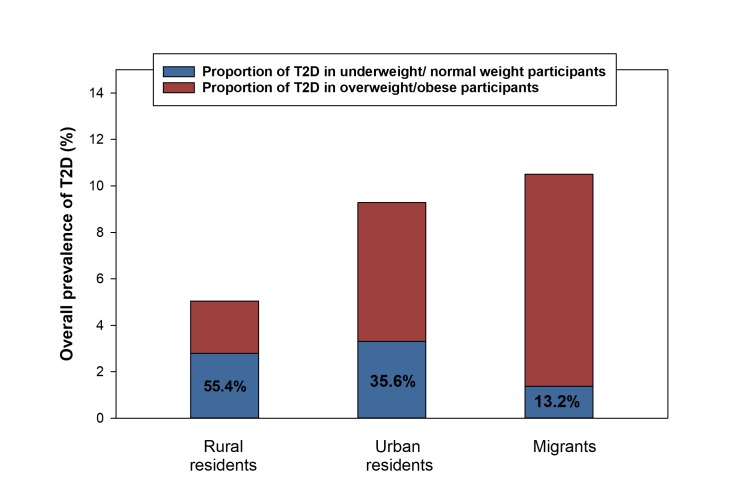
Results: Prevalence of type 2 diabetes in rural, urban and migrant lean participants were 3.5%, 8.9% and 7.5% respectively, representing 55.4%, 35.6%, 13.2% of all participants with type 2 diabetes. Compared with lean rural participants, the odds of type 2 diabetes were higher in lean urban participants (adjusted OR = 8.81, 95% CI = 6.56-11.06), followed by migrants (5.27, 95% CI = 3.51-6.91). Irrespective of site, determinants of type 2 diabetes in lean participants include; presence of hypertension, physical inactivity, hypercholesterolemia and age (>45 years).
Conclusions: Our study shows a high prevalence of type 2 diabetes among lean African populations in different geographical settings. Future studies are needed in-order to examine how contextual differences are related to the pathophysiology of type 2 diabetes in lean individuals.
Copyright © 2019 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Competing interests: The authors completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflicts of interest.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
