

Intrafraction 4D-cone beam CT acquired during volumetric arc radiotherapy delivery: kV parameter optimization and 4D motion accuracy for lung stereotactic body radiotherapy (SBRT) patients
- PMID: 31675150
- PMCID: PMC6909121
- DOI: 10.1002/acm2.12755
Intrafraction 4D-cone beam CT acquired during volumetric arc radiotherapy delivery: kV parameter optimization and 4D motion accuracy for lung stereotactic body radiotherapy (SBRT) patients
Abstract
Purpose: Elekta XVI 5.0 allows for four-dimensional cone beam computed tomography (4D CBCT) image acquisition during treatment delivery to monitor intrafraction motion. These images can have poorer image quality due to undersampling of kV projections and treatment beam MV scatter effects. We determine if a universal intrafraction preset can be used for stereotactic body radiotherapy (SBRT) lung patients and validate the accuracy of target motion characterized by XVI intrafraction 4D CBCT.
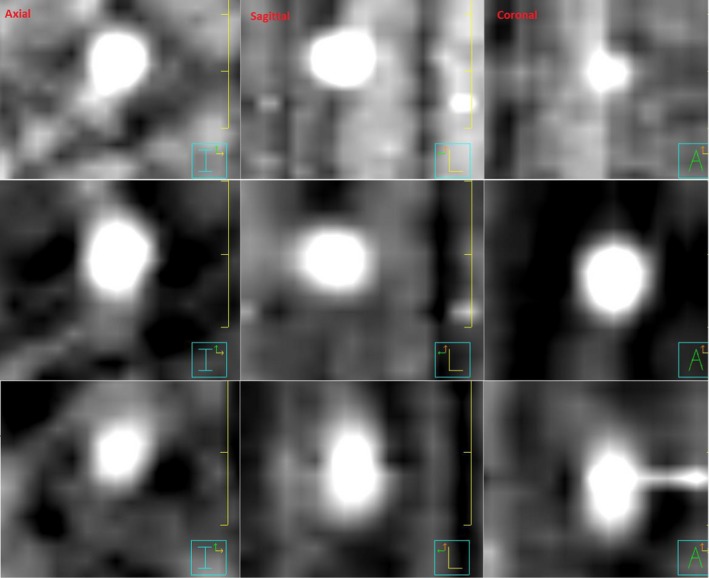
Methods: The most critical parameter within the intrafraction preset is the nominal AcquisitionInterval, which controls kV imaging acquisition frequency. An optimal value was determined by maximizing the kV frame number acquired up to 1000 frames, typical of pretreatment 4D CBCT. CIRS motion phantom intrafraction phase images for 16 SBRT beams were obtained. Mean target position, time-weighted standard deviation, and amplitude for these images as well as target motion for three SBRT lung patients were compared to respective pretreatment 4D CBCTs. Evaluation of intrafraction 4D CBCT reconstruction revealed inclusion of MV only images acquired to remove MV scatter effects. A workaround to remove these images was developed.
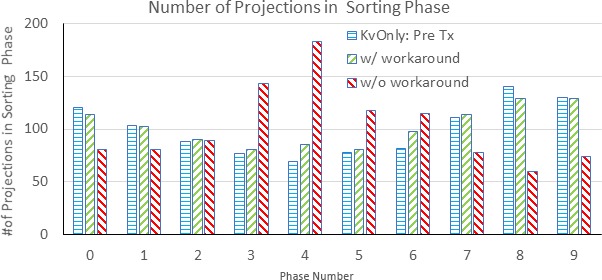
Results: AcquisitionInterval of 0.1°/frame was optimal. The number of kV frames acquired was 567-1116 and showed strong linear correlation with beam monitor unit (MUs). Phantom target motion accuracy was excellent with average differences in target position, standard deviation and amplitude range of ≤0.5 mm. Target tracking for SBRT patients also showed good agreement. Evaluation of phase sorting wave forms showed that inclusion of MV only images significantly impacts intrafraction image reconstruction for patients and use of workaround is necessary.
Conclusions: A universal intrafraction imaging preset can be used safely for SBRT lung patients. The number of kV projections with MV delivery parameters varies; however images with fewer kV projections still provided accurate target position information. Impact of the reconstruction workaround was significant and is mandated for all 4D CBCT intrafraction imaging performed at our institution.
Keywords: 4D CBCT; SBRT; intrafraction; motion validation.
© 2019 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no relevant conflict of interest to disclose.
Figures









References
-
- Sonke JJ, Zijp L, Remeijer P, Van Herk M. Respiratory correlated cone beam CT. Med Phys. 2005;32:1176–1186. - PubMed
-
- Purdie TG, Moseley DJ, Bissonnette JP, et al. Respiration correlated cone‐beam computed tomography and 4DCT for evaluating target motion in Stereotactic Lung Radiation Therapy. Acta Oncol (Madr). 2006;45:915–922. - PubMed
-
- Sonke JJ, Rossi M, Wolthaus J, van Herk M, Damen E, Belderbos J. Frameless stereotactic body radiotherapy for lung cancer using four‐dimensional cone beam CT guidance. Int J Radiat Oncol Biol Phys. 2009;74:567–574. - PubMed
-
- Ford E, Mageras G, Yorke E, Rosenzweig K, Wagman R, Ling C. Evaluation of respiratory movement during gated radiotherapy using film and electronic portal imaging. Int J Radiat Oncol. 2002;52:522–531. - PubMed
-
- Pan T, Lee T‐Y, Rietzel E, Chen GTY. 4D‐CT imaging of a volume influenced by respiratory motion on multi‐slice CT. Med Phys. 2004;31:333–340. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
