

Lesion-Level Response Dynamics to Programmed Cell Death Protein (PD-1) Blockade
- PMID: 31675272
- PMCID: PMC7194449
- DOI: 10.1200/JCO.19.00709
Lesion-Level Response Dynamics to Programmed Cell Death Protein (PD-1) Blockade
Abstract
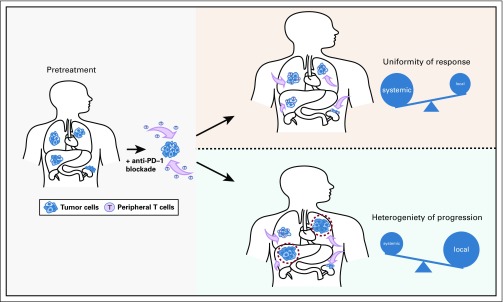
Purpose: Response to programmed cell death protein 1 (PD-1) blockade is often conceptualized as resulting from reinvigoration of tumor-infiltrating lymphocytes. However, recruited antitumor immunity from the periphery may also be an important contributor to response. A detailed assessment of the response dynamics of individual metastasis could provide insight to the systemic and local features that mediate response and resistance to immunotherapy.
Materials and methods: Patients with metastatic non-small-cell lung cancer (NSCLC) or mismatch repair deficiency (MMRD) carcinoma treated with PD-1 monotherapy were evaluated independently. Absolute and percent change of each target lesion were quantified at each computed tomography scan using RECIST. Patterns of progression were predefined as systemic or mixed and were correlated with clinical outcomes.
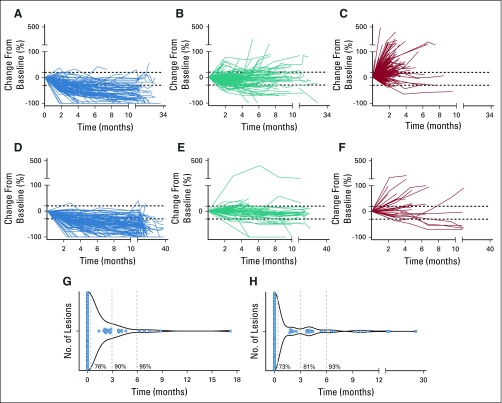
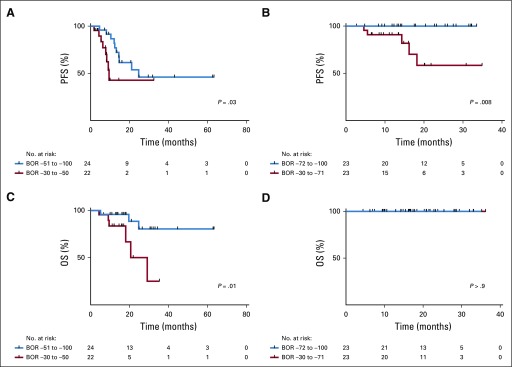
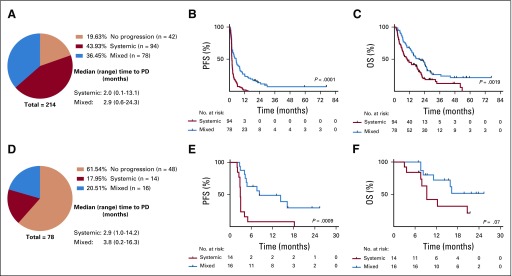
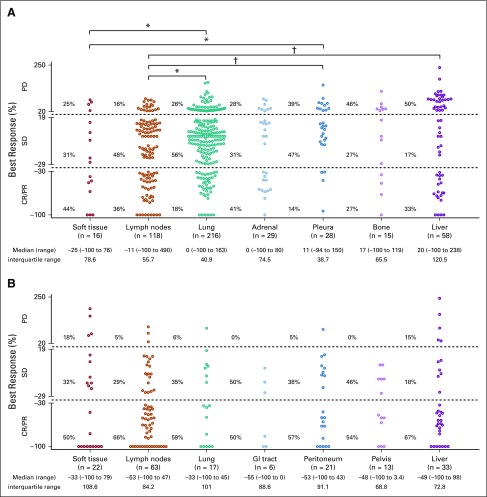
Results: A total of 761 individual lesions from 214 patients with NSCLC and 290 lesions from 78 patients with MMRD carcinoma were examined. Individual target lesion responses aligned with best overall response of each patient (85% NSCLC and 93% MMRD lesions responded in patients with partial response/complete response). In responding patients, timing of response was uniform (73% NSCLC and 76% MMRD lesions responded synchronously), and deeper responses were associated with prolonged progression-free survival and overall survival. By contrast, at progression, mixed progression was common (45% of NSCLC and 53% of MMRD) and associated with improved survival compared with those who experienced systemic progression (NSCLC hazard ratio [HR], 0.58; P = .001; MMRD HR, 0.40; P = .07). Organ sites had differential responses, with lymph node and liver metastasis among the most and least responsive, respectively.
Conclusion: Temporal-spatial patterns of response across individual metastases tend to be uniform, favoring the role of peripheral, clonally directed antitumor immunity as a key mediator of response to PD-1 blockade. In contrast, progression is more heterogeneous, potentially revealing the clinical importance of local features and intertumoral heterogeneity.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
