

Gene Variants That Affect Levels of Circulating Tumor Markers Increase Identification of Patients With Pancreatic Cancer
- PMID: 31676359
- PMCID: PMC7166164
- DOI: 10.1016/j.cgh.2019.10.036
Gene Variants That Affect Levels of Circulating Tumor Markers Increase Identification of Patients With Pancreatic Cancer
Abstract
Background & aims: Levels of carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and cancer antigen 125 (CA-125) in blood are used as markers to determine the response of patients with cancer to therapy, but are not used to identify patients with pancreatic cancer.
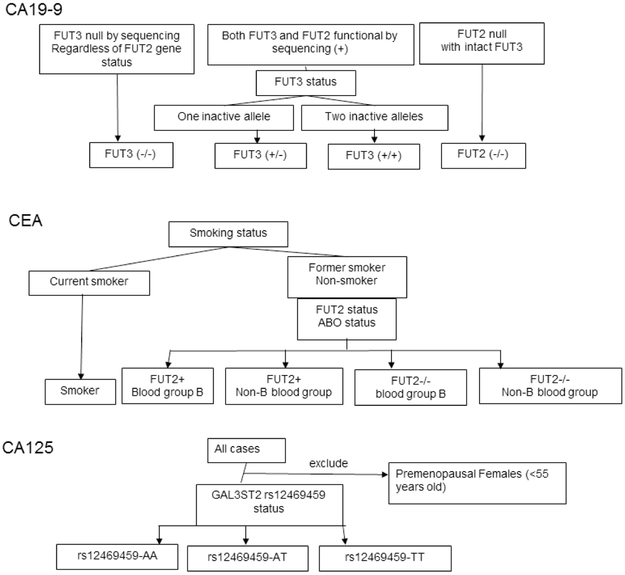
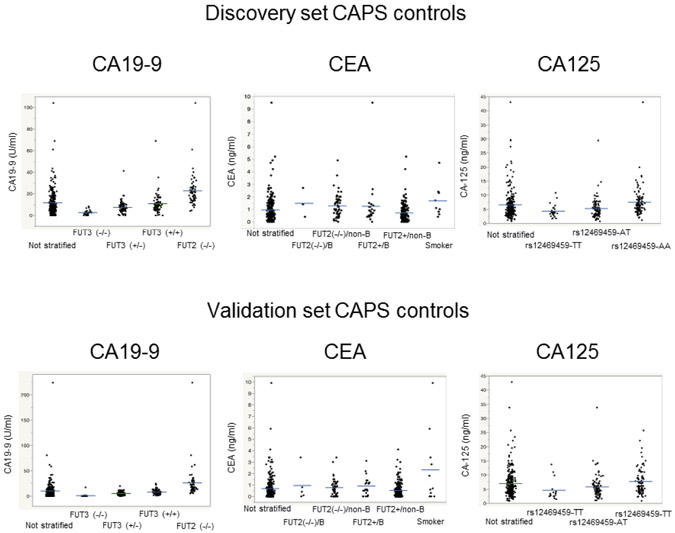
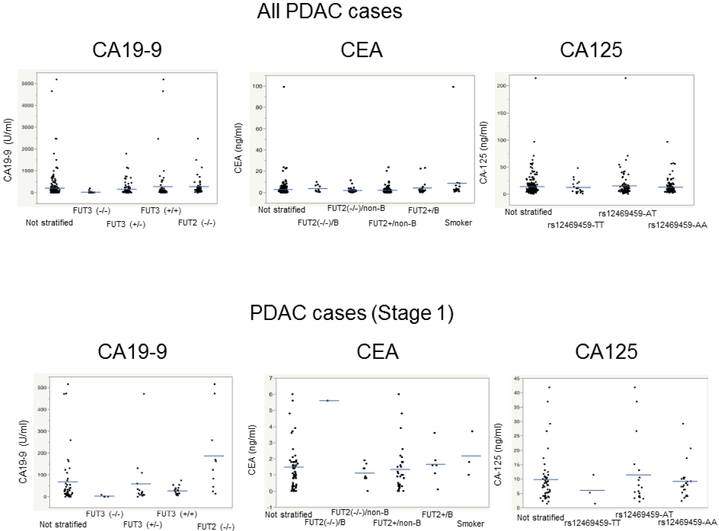
Methods: We obtained blood samples from 504 patients undergoing pancreatic surveillance from 2002 through 2018 who did not develop pancreatic cancer and measured levels of the tumor markers CA19-9, CEA, CA-125, and thrombospondin-2. Single-nucleotide polymorphisms (SNPs) in FUT3, FUT2, ABO, and GAL3ST2 that have been associated with levels of tumor markers were used to establish SNP-defined ranges for each tumor marker. We also tested the association between additional SNPs (in FUT6, MUC16, B3GNT3, FAM3B, and THBS2) with levels of tumor markers. To calculate the diagnostic specificity of each SNP-defined range, we assigned the patients under surveillance into training and validation sets. After determining the SNP-defined ranges, we determined the sensitivity of SNP-adjusted tests for the tumor markers, measuring levels in blood samples from 245 patients who underwent resection for pancreatic ductal adenocarcinoma (PDAC) from 2010 through 2017.
Results: A level of CA19-9 that identified patients with PDAC with 99% specificity had 52.7% sensitivity. When we set the cut-off levels of CA19-9 based on each SNP, the test for CA19-9 identified patients with PDAC with 60.8% sensitivity and 98.8% specificity. Among patients with FUT3 alleles that encode a functional protein, levels of CA19-9 greater than the SNP-determined cut-off values identified 66.4% of patients with PDAC, with 99.3% specificity. In the validation set, levels of CEA varied among patients with vs without SNP in FUT2, by blood group, and among smokers vs nonsmokers; levels of CA-125 varied among patients with vs without the SNP in GAL3ST2. The use of the SNPs to define the ranges of CEA and CA-125 did not significantly increase the diagnostic accuracy of the assays for these proteins. Combining data on levels of CA19-9 and CEA, CA19-9 and CA-125, or CA19-9 and thrombospondin-2 increased the sensitivity of detection of PDAC, but slightly reduced specificity.
Conclusions: Including information on SNPs associated with levels of CA19-9, CEA, and CA-125 can improve the diagnostic accuracy of assays for these tumor markers in the identification of patients with PDAC. Clinicaltrials.gov no: NCT02000089.
Keywords: Diagnosis; Early Detection; Genotype; Screening.
Copyright © 2020 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors do not have any personal or financial conflicts of interest.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA: a cancer journal for clinicians. 2019;69(1):7–34. - PubMed
-
- Vasen H, Ibrahim I, Ponce CG, et al. Benefit of Surveillance for Pancreatic Cancer in High-Risk Individuals: Outcome of Long-Term Prospective Follow-Up Studies From Three European Expert Centers. J Clin Oncol. 2016;34:2010–9. - PubMed
-
- Konings IC, Harinck F, Poley JW, et al. Prevalence and Progression of Pancreatic Cystic Precursor Lesions Differ Between Groups at High Risk of Developing Pancreatic Cancer. Pancreas. 2017;46:28–34. - PubMed
-
- Verna EC, Hwang C, Stevens PD, et al. Pancreatic cancer screening in a prospective cohort of high-risk patients: a comprehensive strategy of imaging and genetics. Clinical Cancer Res. 2010;16(20):5028–37. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
