

18F-DCFPyL PET/CT Imaging in Patients with Biochemically Recurrent Prostate Cancer After Primary Local Therapy
- PMID: 31676732
- PMCID: PMC9374042
- DOI: 10.2967/jnumed.119.234799
18F-DCFPyL PET/CT Imaging in Patients with Biochemically Recurrent Prostate Cancer After Primary Local Therapy
Abstract
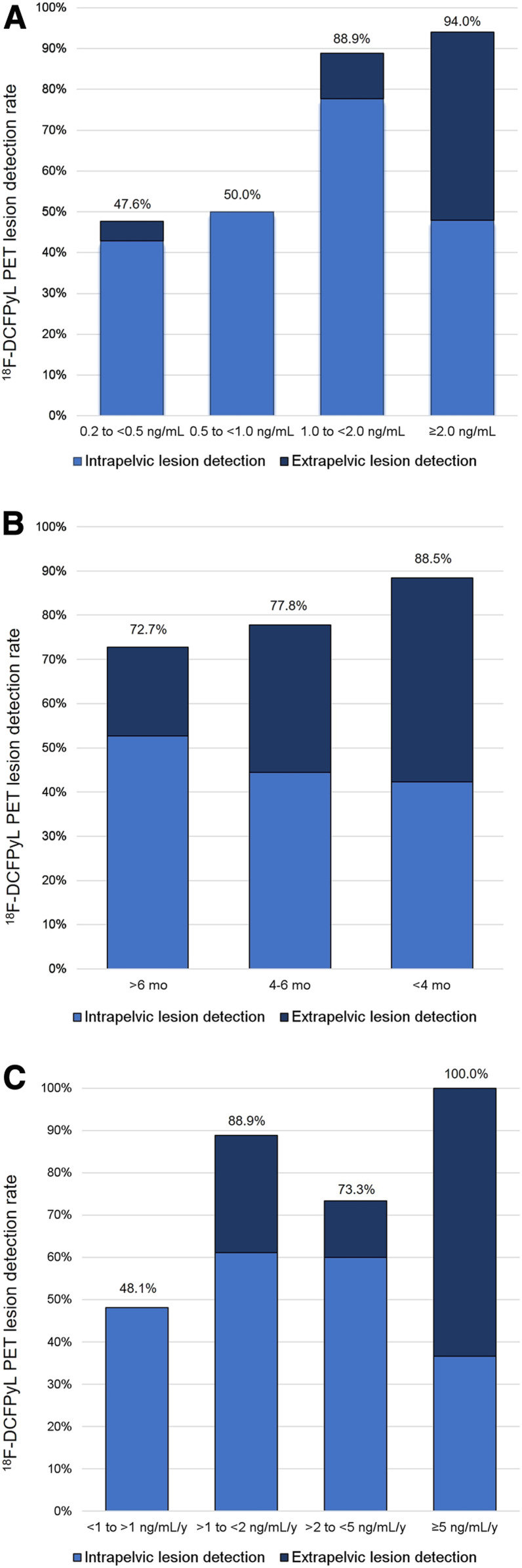
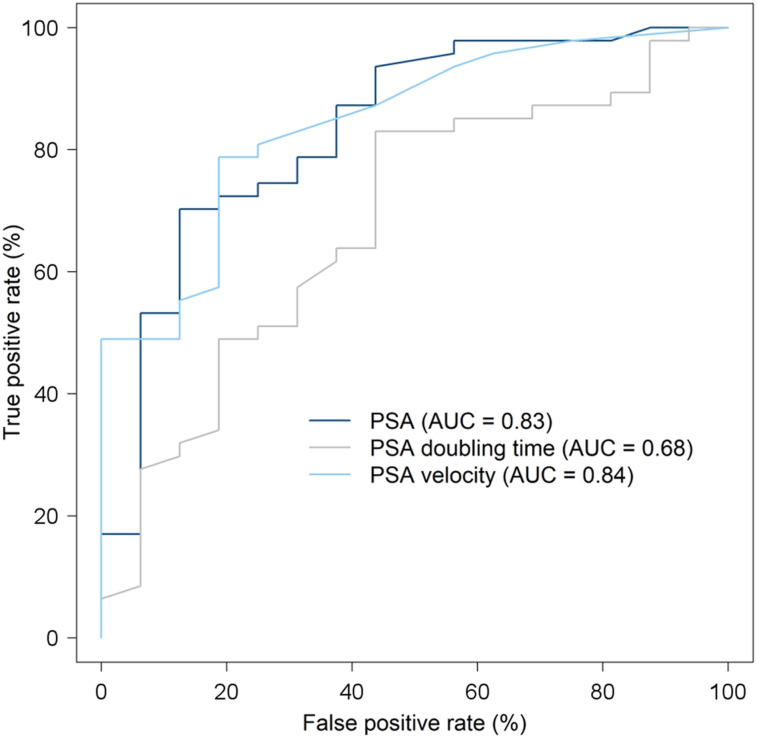
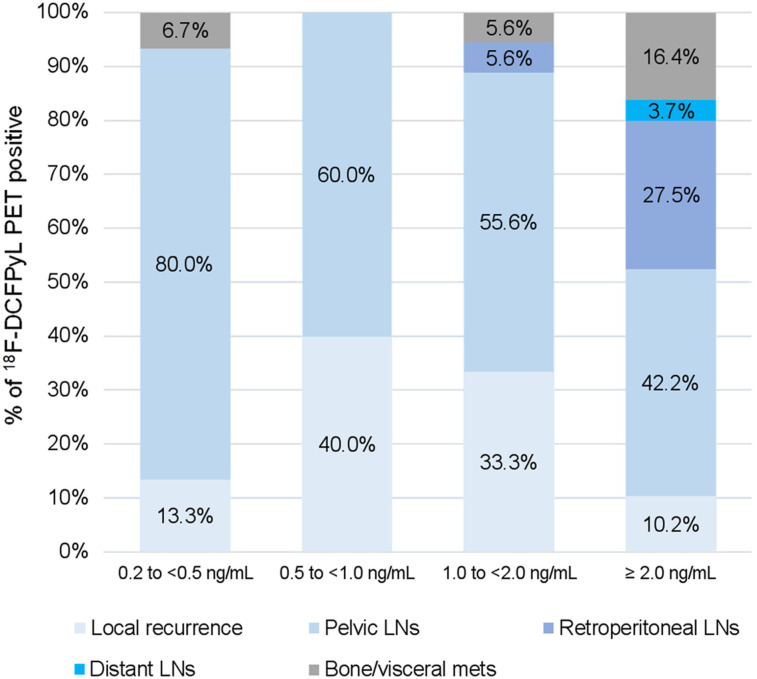
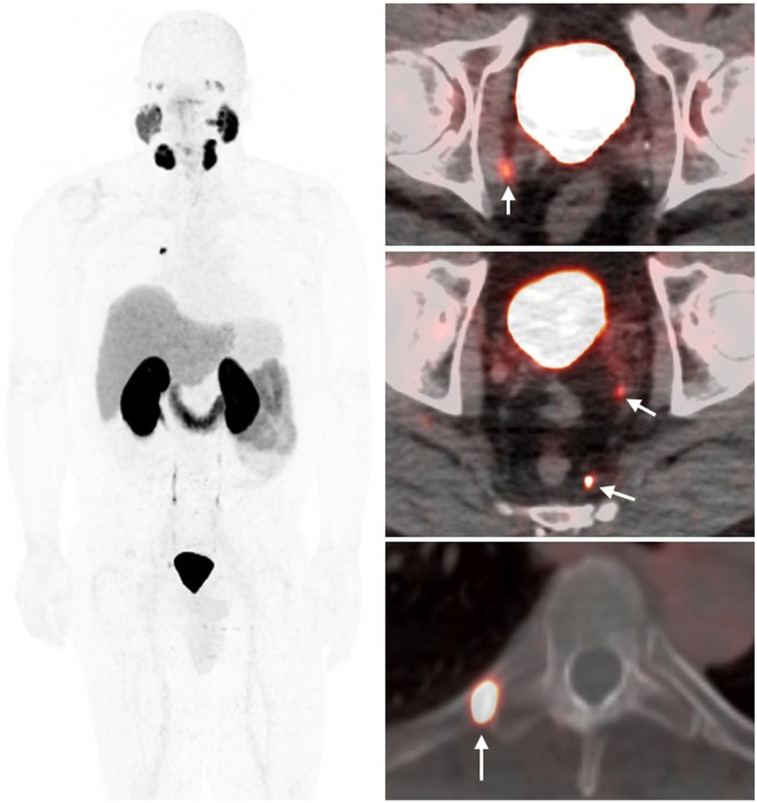
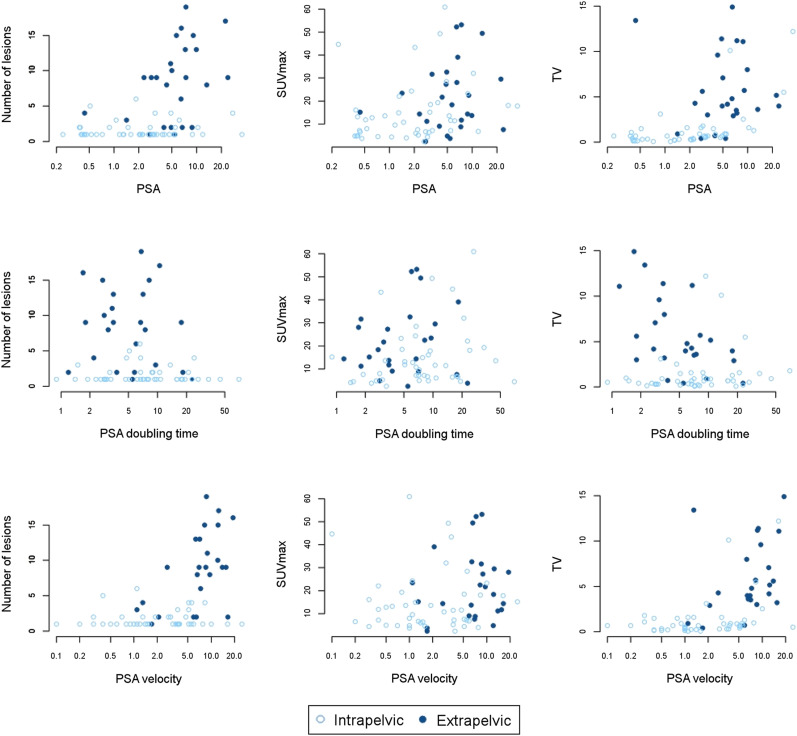
Our objective was to investigate the lesion detection rate of 18F-DCFPyL PET/CT, a prostate-specific membrane antigen (PSMA)-targeted PET agent, in patients with biochemically relapsed prostate cancer after primary local therapy. Methods: This was a prospective institutional review board-approved study of 90 patients with documented biochemical recurrence (median prostate-specific antigen [PSA], 2.5 ng/mL; range, 0.21-35.5 ng/mL) and negative results on conventional imaging after primary local therapies, including radical prostatectomy (n = 38), radiation (n = 27), or a combination of the two (n = 25). Patients on androgen deprivation therapy were excluded. Patients underwent whole-body 18F-DCFPyL PET/CT (299.9 ± 15.5 MBq) at 2 h after injection. The PSMA PET lesion detection rate was correlated with PSA, PSA kinetics, and original primary tumor grade. Results: Seventy patients (77.8%) showed positive PSMA PET results, with a total of 287 lesions identified: 37 prostate bed foci, 208 lesions in lymph nodes, and 42 in distant sites in bones or organs, Eleven patients had negative results, and 9 patients showed indeterminate lesions, which were considered negative in this study. The detection rates were 47.6% (n = 10/21), 50% (n = 5/10), 88.9% (n = 8/9), and 94% (n = 47/50) for PSA levels of >0.2 to <0.5, 0.5 to <1.0, 1 to <2.0, and ≥2.0 ng/mL, respectively. In postsurgical patients, PSA, PSA doubling time, and PSA velocity correlated with PET results, but the same was not true for postradiation patients. These parameters also correlated with the extent of disease on PET (intrapelvic vs. extrapelvic). There was no significant difference in the rate of positive scans between patients with higher-grade and lower-grade primary tumors (Gleason score of ≥4 + 3 vs. <3 + 4). Tumor recurrence was histology-confirmed in 40% (28/70) of patients. On a per-patient basis, positive predictive value was 93.3% (95% confidence interval, 77.6%-99.2%) by histopathologic validation and 96.2% (95% confidence interval, 86.3%-99.7%) by the combination of histology and imaging/clinical follow-up. Conclusion:18F-DCFPyL PET/CT imaging offers high detection rates in biochemically recurrent prostate cancer patients and is positive in about 50% of patients with a PSA level of less than 0.5 ng/mL, which could substantially impact clinical management. In postsurgical patients, 18F-DCFPyL PET/CT correlates with PSA, PSA doubling time, and PSA velocity, suggesting it may have prognostic value. 18F-DCFPyL PET/CT is highly promising for localizing sites of recurrent prostate cancer.
Keywords: DCFPyL; PET; PSMA; biochemical recurrence; prostate cancer.
© 2020 by the Society of Nuclear Medicine and Molecular Imaging.
Figures

References
-
- Mottet N, Bellmunt J, Bolla M, et al. EAU guidelines on prostate cancer. Part II: treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol. 2011;59:572–583. - PubMed
-
- Pfister D, Bolla M, Briganti A, et al. Early salvage radiotherapy following radical prostatectomy. Eur Urol. 2014;65:1034–1043. - PubMed
-
- Briganti A, Karnes RJ, Gandaglia G, et al. Natural history of surgically treated high-risk prostate cancer. Urol Oncol. 2015;33:163 e167-113. - PubMed
-
- Freedland SJ, Humphreys EB, Mangold LA, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA. 2005;294:433–439. - PubMed
-
- Beer AJ, Eiber M, Souvatzoglou M, Schwaiger M, Krause BJ. Radionuclide and hybrid imaging of recurrent prostate cancer. Lancet Oncol. 2011;12:181–191. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous