

Platform for ergonomic intraoral photodynamic therapy using low-cost, modular 3D-printed components: Design, comfort and clinical evaluation
- PMID: 31676807
- PMCID: PMC6825190
- DOI: 10.1038/s41598-019-51859-6
Platform for ergonomic intraoral photodynamic therapy using low-cost, modular 3D-printed components: Design, comfort and clinical evaluation
Abstract
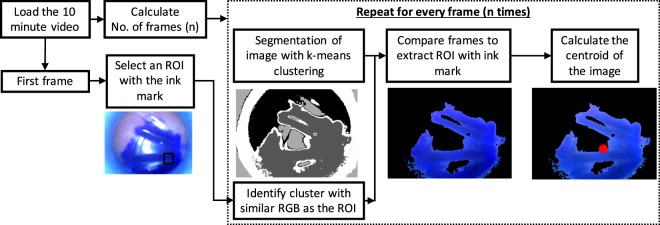
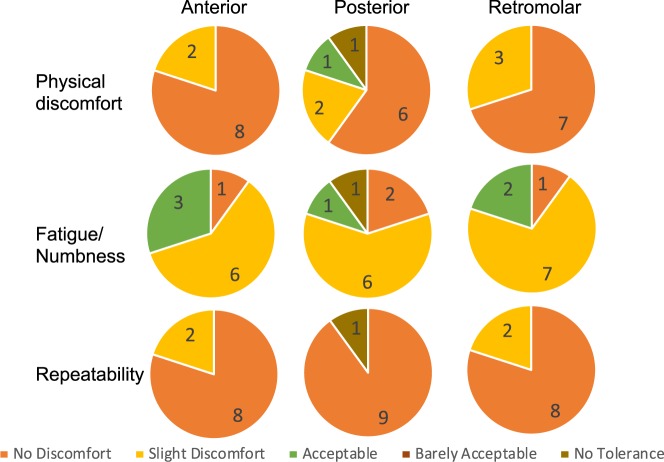
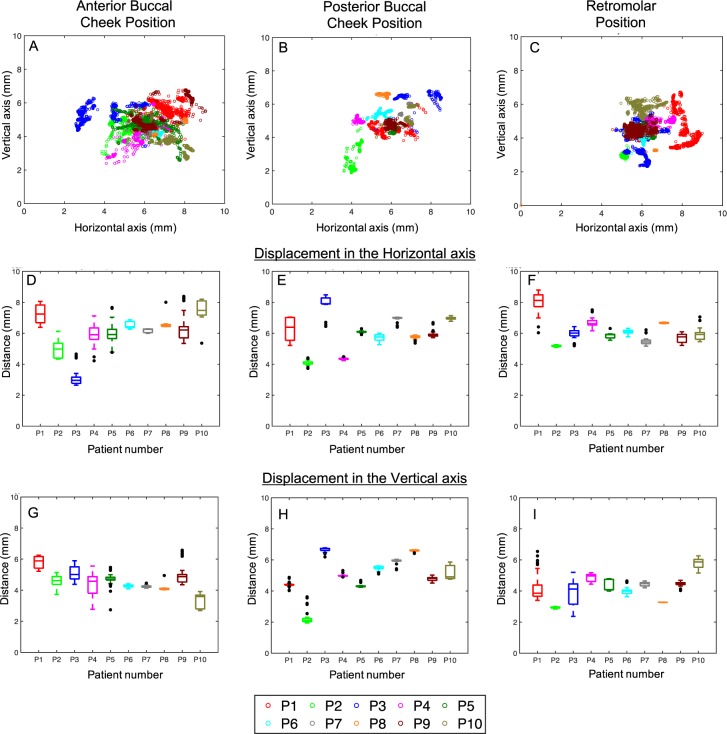
Oral cancer prevalence is increasing at an alarming rate worldwide, especially in developing countries which lack the medical infrastructure to manage it. For example, the oral cancer burden in India has been identified as a public health crisis. The high expense and logistical barriers to obtaining treatment with surgery, radiotherapy and chemotherapy often result in progression to unmanageable late stage disease with high morbidity. Even when curative, these approaches can be cosmetically and functionally disfiguring with extensive side effects. An alternate effective therapy for oral cancer is a light based spatially-targeted cytotoxic therapy called photodynamic therapy (PDT). Despite excellent healing of the oral mucosa in PDT, a lack of robust enabling technology for intraoral light delivery has limited its broader implementation. Leveraging advances in 3D printing, we have developed an intraoral light delivery system consisting of modular 3D printed light applicators with pre-calibrated dosimetry and mouth props that can be utilized to perform PDT in conscious subjects without the need of extensive infrastructure or manual positioning of an optical fiber. To evaluate the stability of the light applicators, we utilized an endoscope in lieu of the optical fiber to monitor motion in the fiducial markers. Here we showcase the stability (less than 2 mm deviation in both horizontal and vertical axis) and ergonomics of our applicators in delivering light precisely to the target location in ten healthy volunteers. We also demonstrate in five subjects with T1N0M0 oral lesions that our applicators coupled with a low-cost fiber coupled LED-based light source served as a complete platform for intraoral light delivery achieving complete tumor response with no residual disease at initial histopathology follow up in these patients. Overall, our approach potentiates PDT as a viable therapeutic option for early stage oral lesions that can be delivered in low resource settings.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Shield KD, et al. The global incidence of lip, oral cavity, and pharyngeal cancers by subsite in 2012. CA: A Cancer Journal for Clinicians. 2016;67:51–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
