

The role of bacterial skin infections in atopic dermatitis: expert statement and review from the International Eczema Council Skin Infection Group
- PMID: 31677162
- PMCID: PMC7317931
- DOI: 10.1111/bjd.18643
The role of bacterial skin infections in atopic dermatitis: expert statement and review from the International Eczema Council Skin Infection Group
Abstract
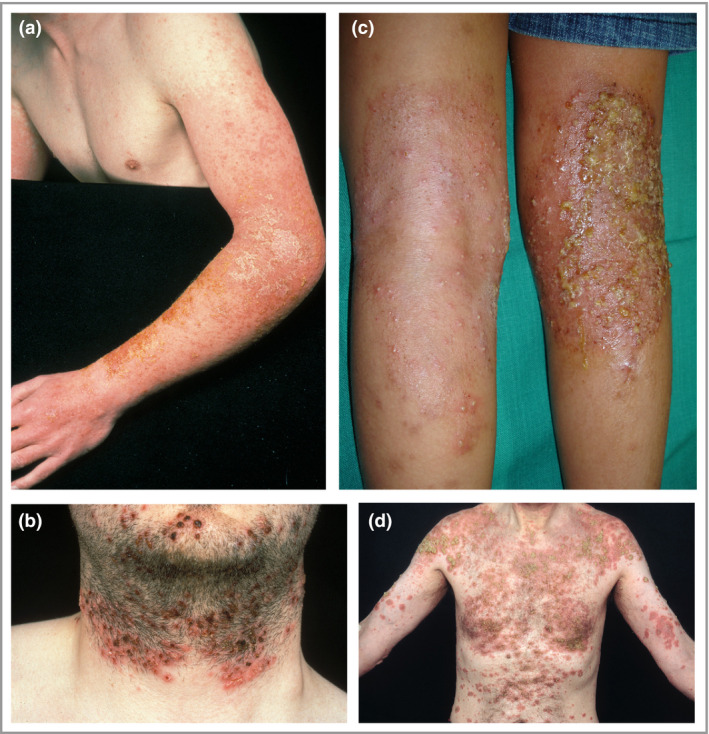
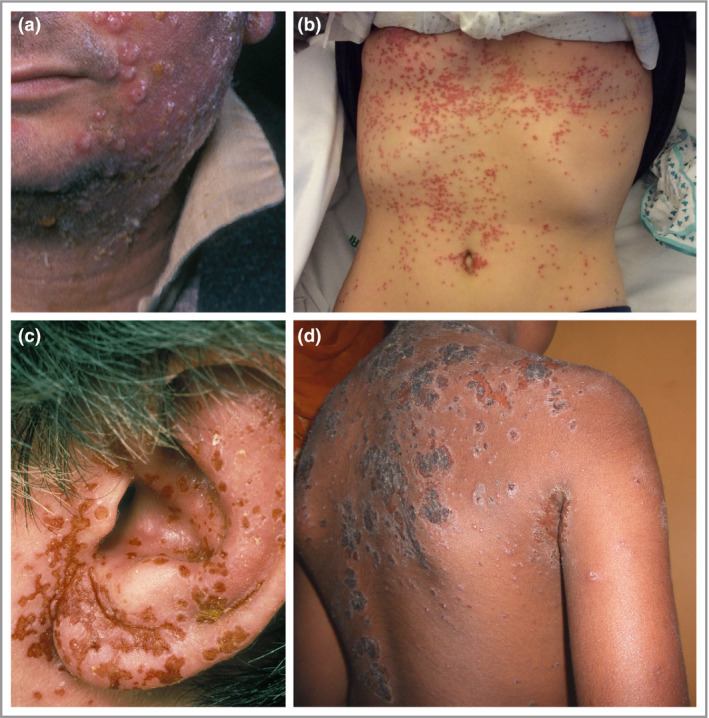
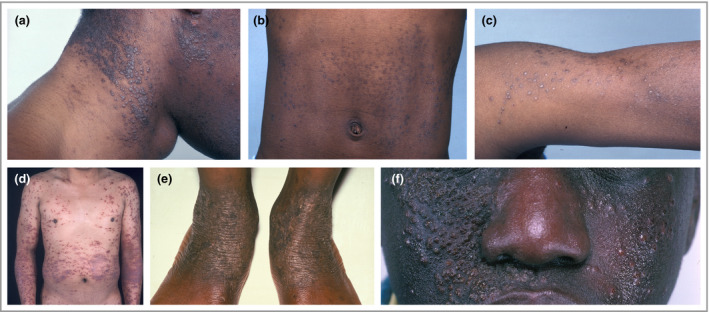
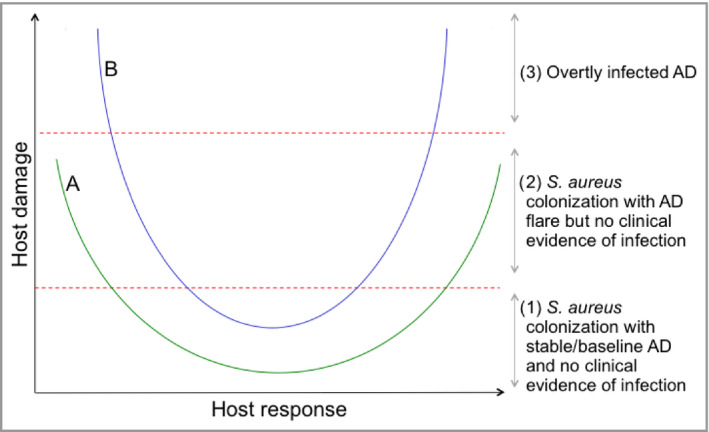
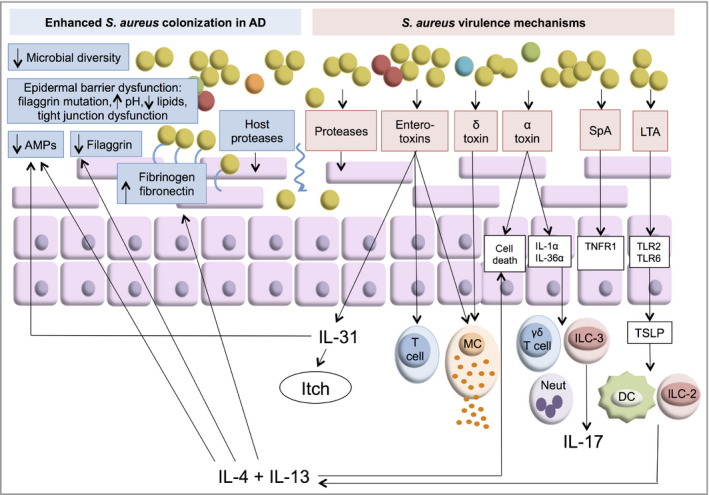
Patients with atopic dermatitis (AD) have an increased risk of bacterial skin infections, which cause significant morbidity and, if untreated, may become systemic. Staphylococcus aureus colonizes the skin of most patients with AD and is the most common organism to cause infections. Overt bacterial infection is easily recognized by the appearance of weeping lesions, honey-coloured crusts and pustules. However, the wide variability in clinical presentation of bacterial infection in AD and the inherent features of AD - cutaneous erythema and warmth, oozing associated with oedema, and regional lymphadenopathy - overlap with those of infection, making clinical diagnosis challenging. Furthermore, some features may be masked because of anatomical site- and skin-type-specific features, and the high frequency of S. aureus colonization in AD makes positive skin swab culture of suspected infection unreliable as a diagnostic tool. The host mechanisms and microbial virulence factors that underlie S. aureus colonization and infection in AD are incompletely understood. The aim of this article is to present the latest evidence from animal and human studies, including recent microbiome research, to define the clinical features of bacterial infections in AD, and to summarize our current understanding of the host and bacterial factors that influence microbial colonization and virulence.
© 2019 The Authors. British Journal of Dermatology published by John Wiley & Sons Ltd on behalf of British Association of Dermatologists.
Figures


References
-
- Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol Suppl 1980; 92:44–7.
-
- Silverberg JI, Silverberg NB. Childhood atopic dermatitis and warts are associated with increased risk of infection: a US population‐based study. J Allergy Clin Immunol 2014; 133:1041–7. - PubMed
-
- Brook I, Frazier EH, Yeager JK. Microbiology of infected atopic dermatitis. Int J Dermatol 1996; 35:791–3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
