Morphology of the Esophageal Hiatus: Is It Different in 3 Types of Hiatus Hernias?
- PMID: 31677612
- PMCID: PMC6955188
- DOI: 10.5056/jnm18208
Morphology of the Esophageal Hiatus: Is It Different in 3 Types of Hiatus Hernias?
Abstract
Background/aims: The esophageal hiatus is formed by the right crus of the diaphragm in the majority of subjects. Contraction of the hiatus exerts a sphincter-like action on the lower esophageal sphincter (LES). The aim is to study the hiatal anatomy (using CT scan imaging) and function (using high-resolution manometry [HRM]), and esophageal motor function in patients with sliding and paraesophageal hiatal hernia.
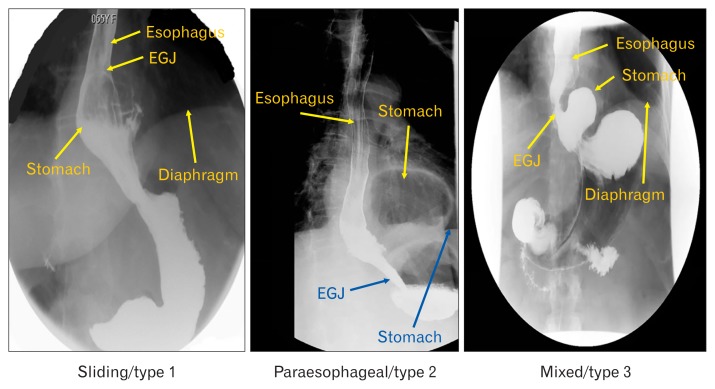
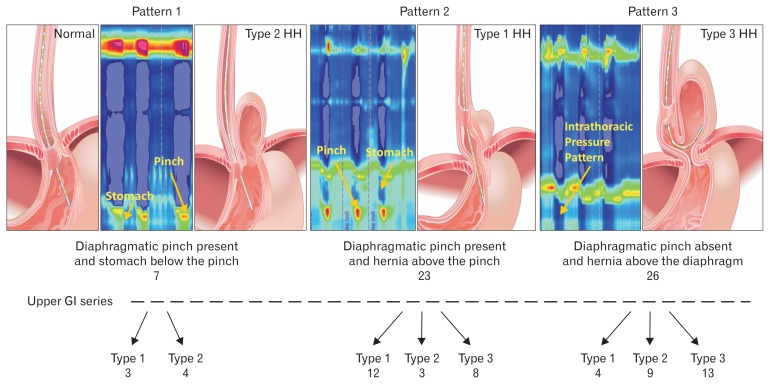
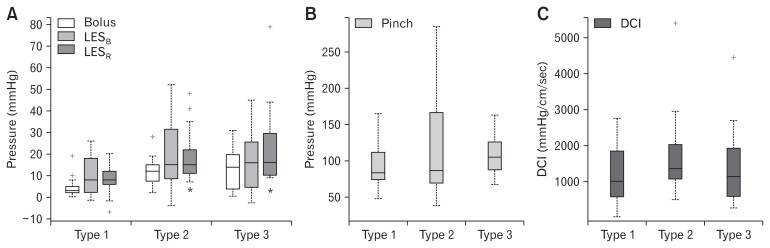
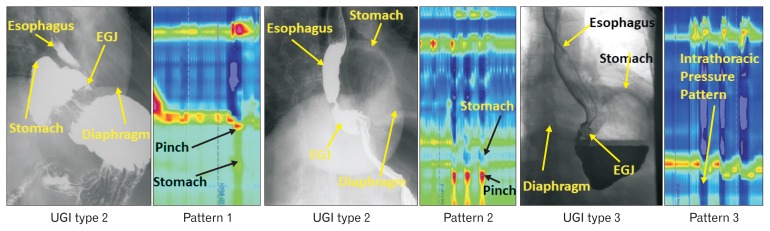
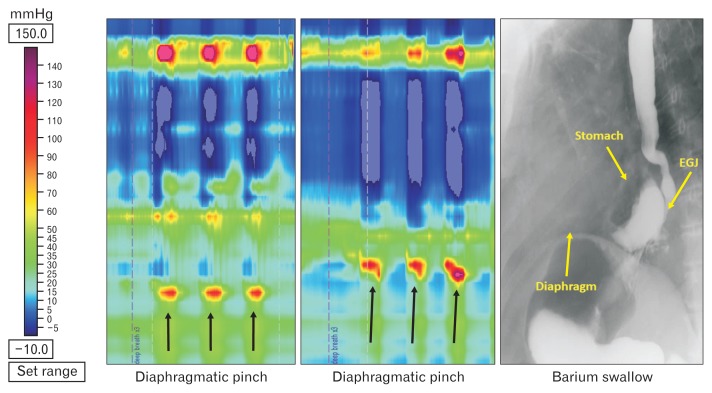
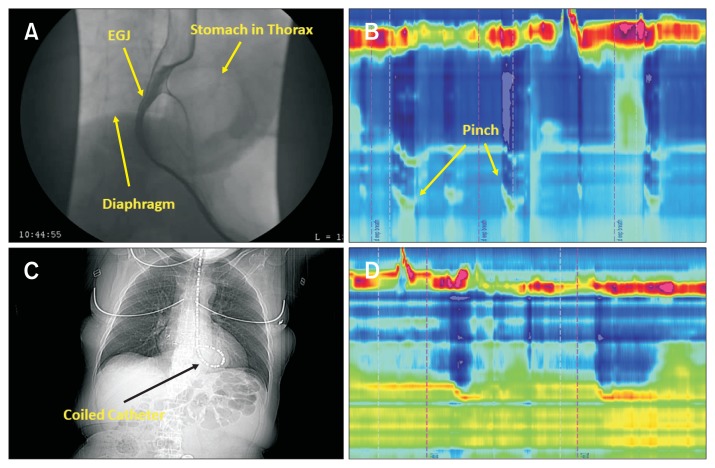
Methods: We assessed normal subjects (n = 20), patients with sliding type 1 hernia (n = 18), paraesophageal type 2 hernia (n = 19), and mixed type 3 hernia (n = 19). Hernia diagnosis was confirmed on the upper gastrointestinal series. The hiatal morphology was constructed from the CT scan images. The LES pressure and relaxation, percent peristalsis, bolus pressure, and hiatal squeeze pressure were assessed by HRM.
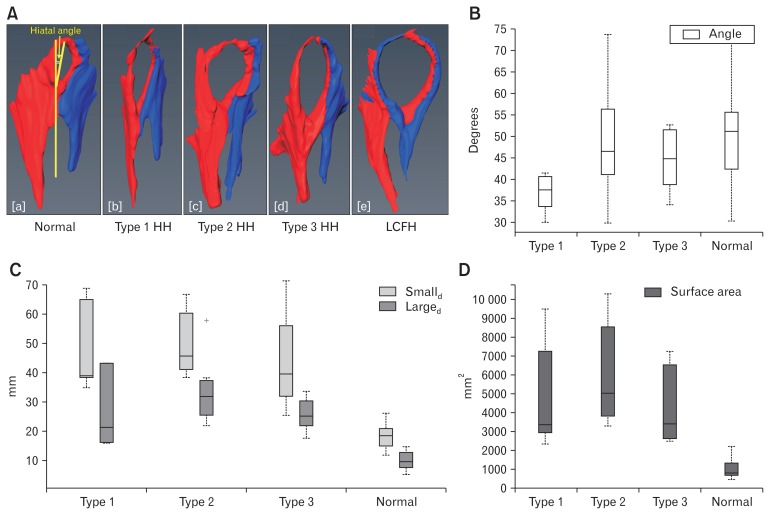
Results: The CT images revealed that the esophageal hiatus is formed by the right crus of the diaphragm in all normal subjects and 86% of hernia patients. The hiatus is elliptical in shape with a surface area of 1037 mm2 in normal subjects. The hiatal dimensions were larger in patients compared to normal subjects. The HRM revealed impaired LES relaxation and higher bolus pressure in patients with paraesophageal compared to the sliding hernia. The hiatal pinch on HRM was recognized in significantly higher number of patients with sliding as compared to paraesophageal hernia.
Conclusions: Using a novel approach, we provide details of the esophageal hiatus in patients with various kinds of hiatal hernia. Impaired LES relaxation in paraesophageal hernia may play a role in its pathophysiology and genesis of symptoms.
Keywords: Esophageal peristalsis; Hiatal; Lower esophageal sphincter; Manometry; Tomography X-ray computed; hernia.
Conflict of interest statement
Figures
References
-
- Listerud MB, Harkins HN. Variations in the muscular anatomy of the esophageal hiatus: based on dissections of two hundred and four fresh cadavers. West J Surg Obstet Gynecol. 1959;67:110–112. discussion 112–113. - PubMed