

Individualized clinical management of patients at risk for Alzheimer's dementia
- PMID: 31677936
- PMCID: PMC6925647
- DOI: 10.1016/j.jalz.2019.08.198
Individualized clinical management of patients at risk for Alzheimer's dementia
Abstract
Introduction: Multidomain intervention for Alzheimer's disease (AD) risk reduction is an emerging therapeutic paradigm.
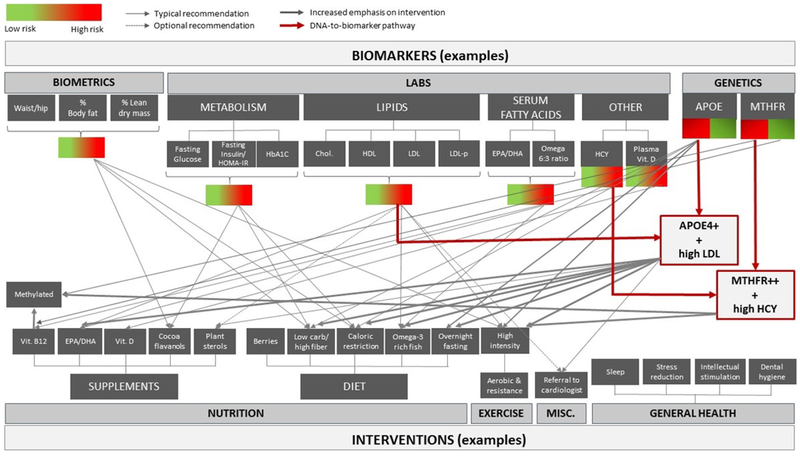
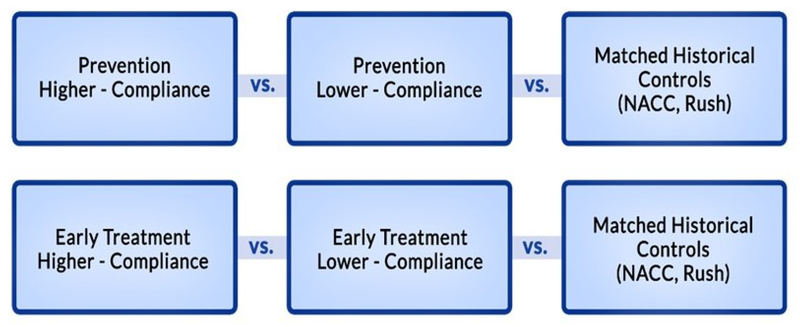
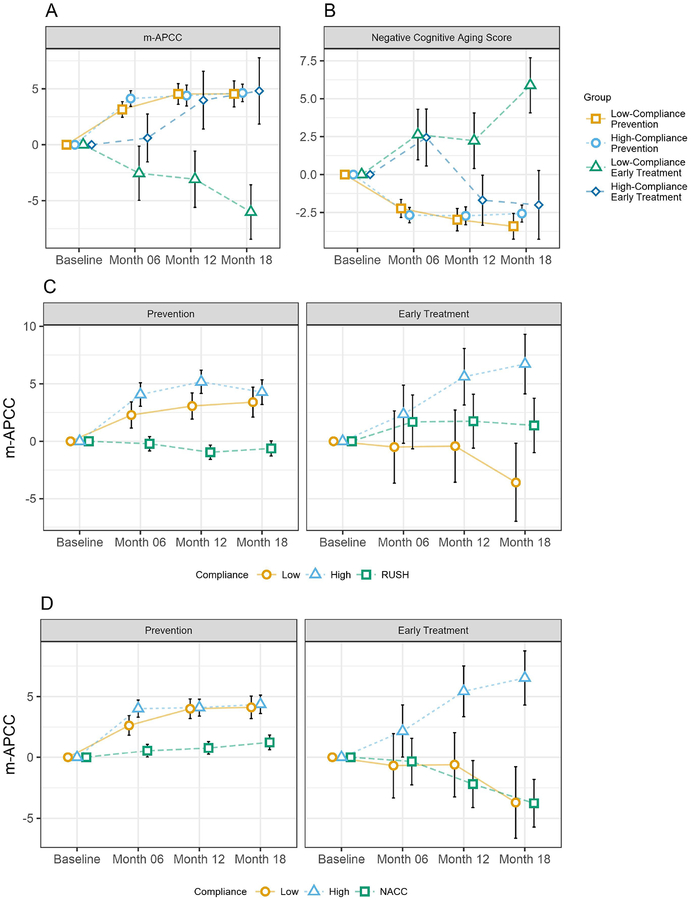
Methods: Patients were prescribed individually tailored interventions (education/pharmacologic/nonpharmacologic) and rated on compliance. Normal cognition/subjective cognitive decline/preclinical AD was classified as Prevention. Mild cognitive impairment due to AD/mild-AD was classified as Early Treatment. Change from baseline to 18 months on the modified Alzheimer's Prevention Cognitive Composite (primary outcome) was compared against matched historical control cohorts. Cognitive aging composite (CogAging), AD/cardiovascular risk scales, and serum biomarkers were secondary outcomes.
Results: One hundred seventy-four were assigned interventions (age 25-86). Higher-compliance Prevention improved more than both historical cohorts (P = .0012, P < .0001). Lower-compliance Prevention also improved more than both historical cohorts (P = .0088, P < .0055). Higher-compliance Early Treatment improved more than lower compliance (P = .0007). Higher-compliance Early Treatment improved more than historical cohorts (P < .0001, P = .0428). Lower-compliance Early Treatment did not differ (P = .9820, P = .1115). Similar effects occurred for CogAging. AD/cardiovascular risk scales and serum biomarkers improved.
Discussion: Individualized multidomain interventions may improve cognition and reduce AD/cardiovascular risk scores in patients at-risk for AD dementia.
Keywords: Alzheimer's disease prevention; Alzheimer's prevention clinic; Multi-domain interventions; Personalized medicine; Preclinical Alzheimer's disease.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests
The authors report no conflicts of interest or other relevant disclosures.
Figures
References
-
- Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s & dementia: the journal of the Alzheimer’s Association 2011; 7(3): 280–92. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
