

Diagnostic Performance of Three-Dimensional Endothelium/Descemet Membrane Complex Thickness Maps in Active Corneal Graft Rejection
- PMID: 31678558
- PMCID: PMC7002262
- DOI: 10.1016/j.ajo.2019.10.022
Diagnostic Performance of Three-Dimensional Endothelium/Descemet Membrane Complex Thickness Maps in Active Corneal Graft Rejection
Abstract
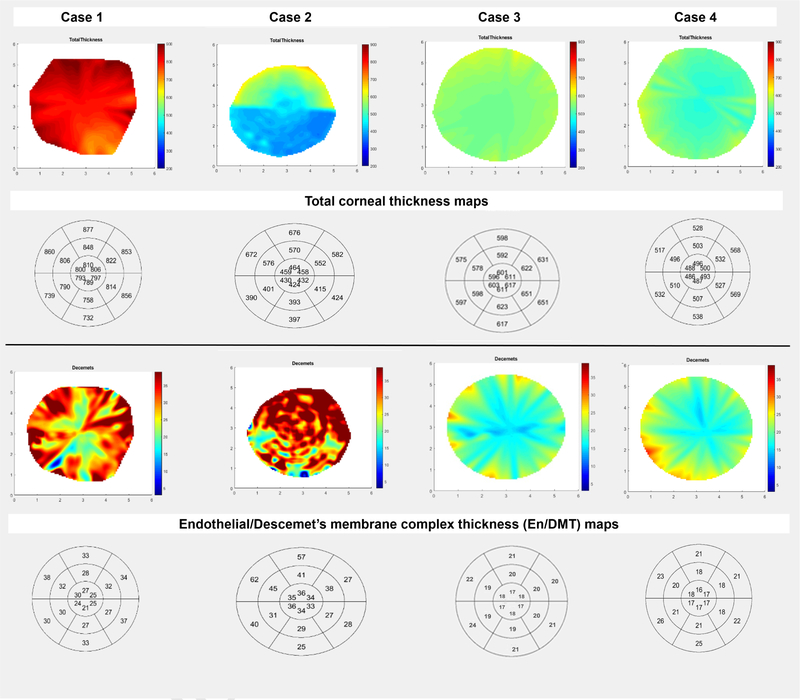
Purpose: To evaluate the performance of 3-dimensional (3D) endothelium/Descemet membrane complex thickness (En/DMT) maps vs total corneal thickness (TCT) maps in the diagnosis of active corneal graft rejection.
Design: Cross-sectional study.
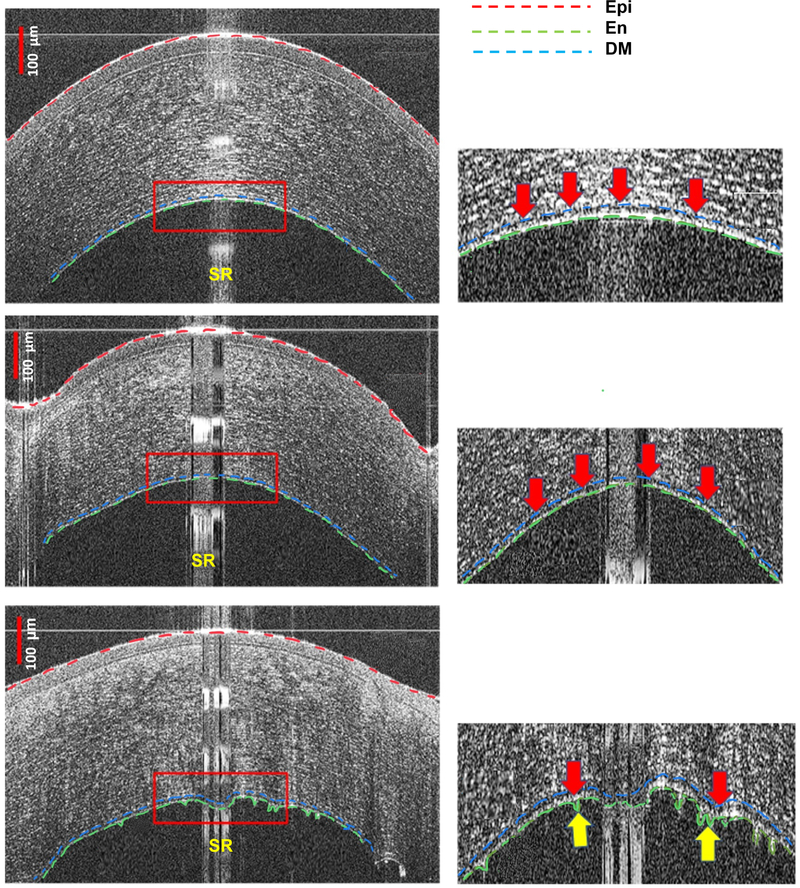
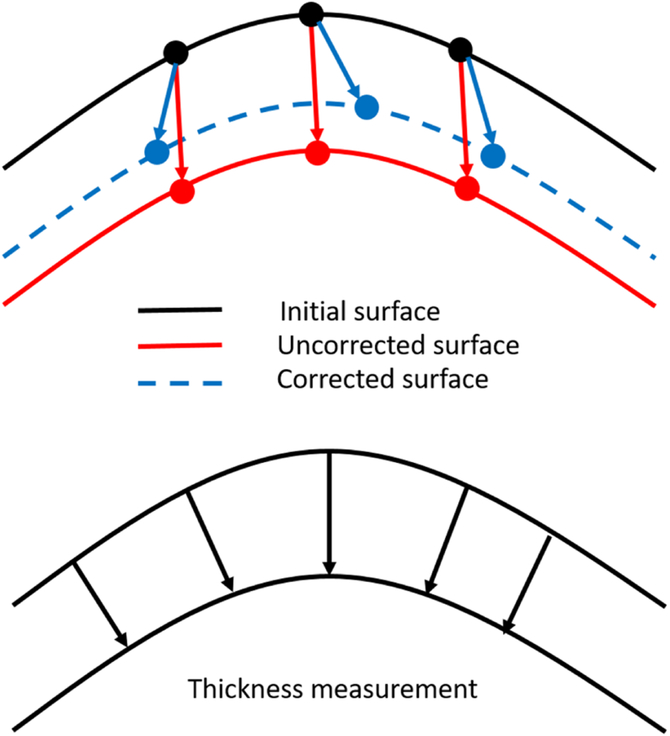
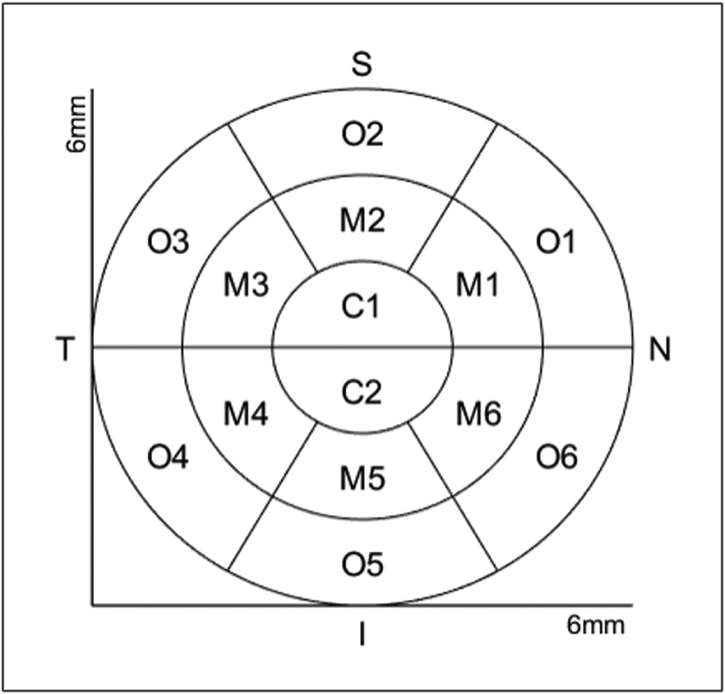
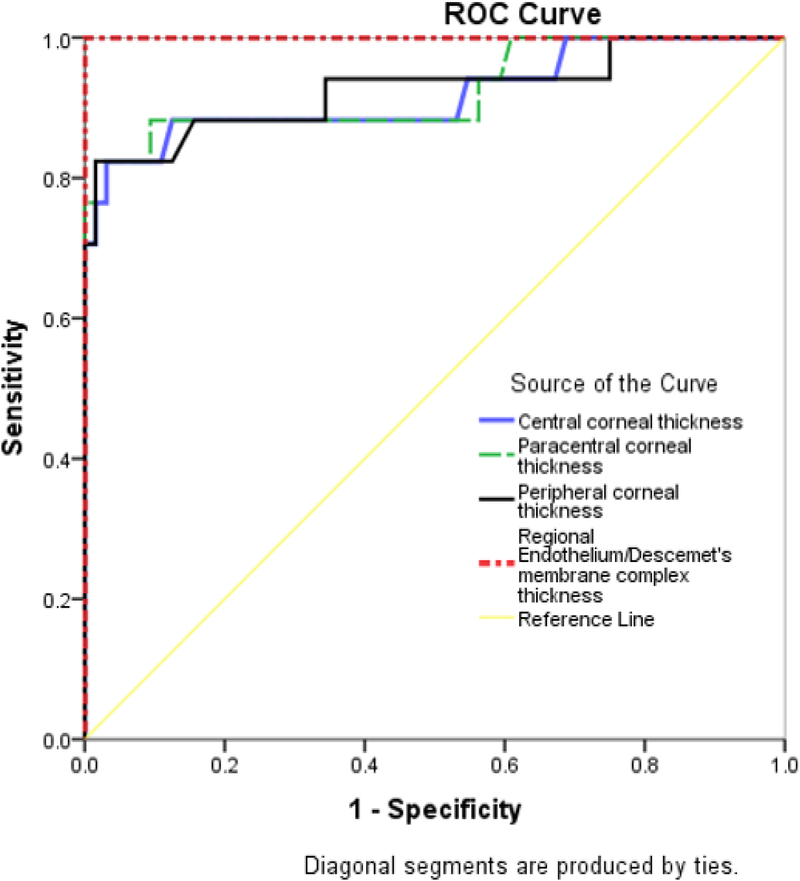
Methods: Eighty-one eyes (32 clear grafts and 17 with active rejection, along with 32 age-matched control eyes) were imaged using high-definition optical coherence tomography (HD-OCT), and a custom-built segmentation algorithm was used to generate 3D color-coded maps of TCT and En/DMT of the central 6-mm cornea. Regional En/DMT and TCT were analyzed and compared between the studied groups. Receiver operating characteristic curves were used to determine the accuracy of En/DMT and TCT maps in differentiating between studied groups. Main outcome measures were regional En/DMT and TCT.
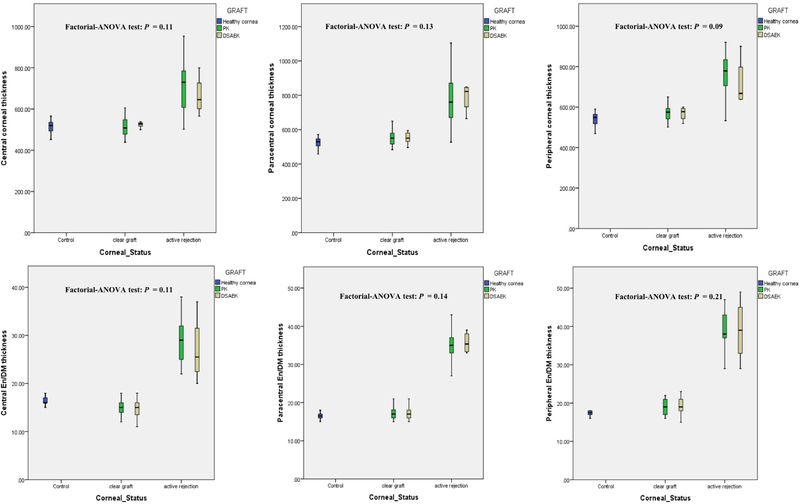
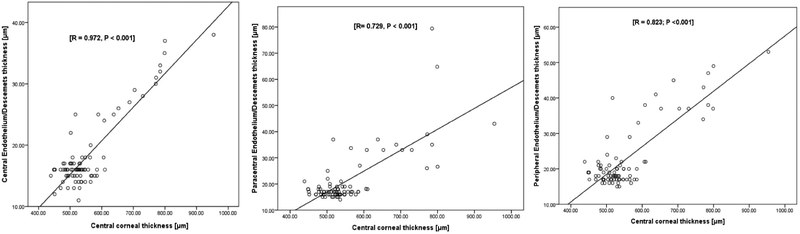
Results: Both regional TCT and En/DMT were significantly greater in actively rejecting grafts compared to both healthy corneas and clear grafts (P < .001). Using 3D thickness maps, central, paracentral, and peripheral En/DMT achieved 100% sensitivity and 100% specificity in diagnosing actively rejecting grafts (optimal cut-off value [OCV] of 19 μm, 24 μm, and 26 μm, respectively), vs only 82% sensitivity and 96% specificity for central TCT, OCV of 587 μm. Moreover, central, paracentral, and peripheral En/DMT correlated significantly with graft rejection severity (r = 0.972, r = 0.729, and r = 0.823, respectively; P < .001).
Conclusion: 3D En/DMT maps can diagnose active corneal graft rejection with excellent accuracy, sensitivity, and specificity. Future longitudinal studies are required to evaluate the predictive and prognostic role of 3D En/DMT maps in corneal graft rejection.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
References
-
- Gain P, Jullienne R, He Z et al. Global Survey of Corneal Transplantation and Eye Banking. JAMA Ophthalmol 2016; 134(2):167–173. - PubMed
-
- Wilson SE, Kaufman HE, Graft failure after penetrating keratoplasty. Surv Ophthalmol 1990; 34(5): 325–356. - PubMed
-
- Musch DC, Schwartz AE, Fitzgerald-Shelton K, Sugar A, Meyer RF. The effect of allograft rejection after penetrating keratoplasty on central endothelial cell density. 1991; 111(6): 739–742. - PubMed
-
- Alldredge OC, Krachmer JH. Clinical types of corneal transplant rejection. Their manifestations, frequency, preoperative correlates, and treatment. Arch Ophthalmol 1981; 99(4): 599–604. - PubMed
-
- Williams KA, Muehlberg SM, Lewis RF et al. How successful is corneal transplantation? A report from the Australian Corneal Graft Register. Eye 1995; 9 (2): 219–227. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
