

Increasing Burden of Hepatitis A in Adolescents and Adults and the Need for Long-Term Protection: A Review from the Indian Subcontinent
- PMID: 31679118
- PMCID: PMC6856242
- DOI: 10.1007/s40121-019-00270-9
Increasing Burden of Hepatitis A in Adolescents and Adults and the Need for Long-Term Protection: A Review from the Indian Subcontinent
Abstract
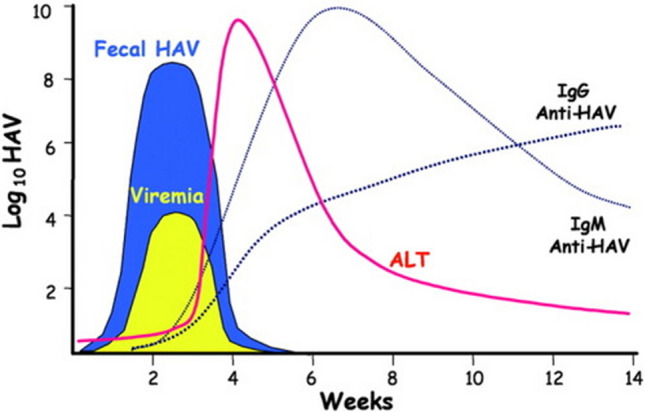
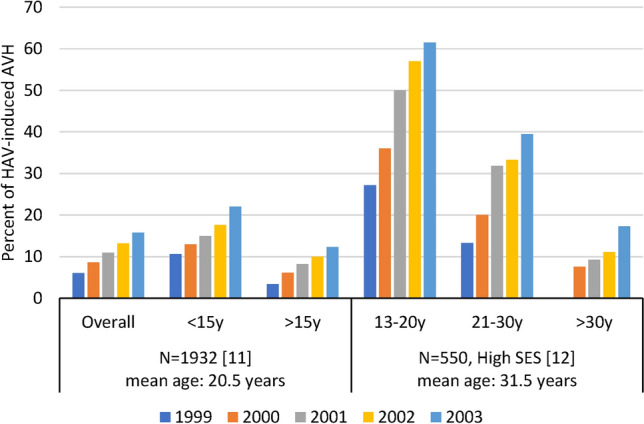
Hepatitis A, an acute inflammatory liver disease caused by hepatitis A virus (HAV) infection from close contact with infected people, is highly endemic in the Indian subcontinent. Due to poor sanitary conditions, most of the population is exposed to the virus in childhood. At this age, the disease is asymptomatic and provides life-long protection against the disease. Due to rapid socioeconomic development in some areas, however, pockets of the population are reaching adolescence/adulthood without prior exposure to the virus and are thus susceptible to infection. At these ages, infection carries a higher risk of symptomatic disease and complications including mortality. This review of epidemiology and burden of disease studies in the Indian subcontinent, published since 2005, shows increasing evidence of a shift from high to intermediate endemicity in high-income-typically urban-populations. The prevalence of anti-HAV antibodies (previously reported at > 90%) is lower now in adolescents and young adults (e.g., around 80% in Bangladesh and 55% in 5-15 years in India). As a result, HAV is responsible for more acute viral hepatitis predominantly in this age group (e.g., > 15 years: 3.4% in 1999 to 12.3% in 2003 or high socioeconomic status 13-20 years: 27% in 1999 to 62% in 2003), with a greater clinical and economic burden. Numerous outbreaks due to HAV have been reported [e.g., Sri Lanka (2009-2010): > 13,000 affected; Kashmir (2015-2017): 12 outbreaks; Kerala (2012-2016): 84 outbreaks] from water or food contamination. Due to current shifts in endemicity, a growing proportion of the population is no longer exposed in childhood. As the disease remains highly endemic, it also provides a source for more severe disease in susceptible people at an older age and for outbreaks. Well-tolerated and effective vaccines are available and help prevent disease burden and provide long-term protection. These should now be used more widely to protect more patients from the growing disease burden of hepatitis A. FUNDING: GlaxoSmithKline Biologicals SA. Plain language summary available for this article-please see Fig. 1 and the following link: https://doi.org/10.6084/m9.figshare.9963044.Fig. 1Plain Language Summary. Highlights the context of the article, the endemicity shift and the burden of hepatitis A in adolescents and adults and steps to be taken to address the impact of this disease.
Keywords: Adolescent; Adult; Asia; Burden; Cost; Epidemiology; Hepatitis A; India; Seroprevalence; Vaccination.
Conflict of interest statement
Ashish Agrawal is an employee of the GSK group of companies. Sanjeev Singh is an employee of the GSK group of companies. Shafi Kolhapure is an employee of the GSK group of companies. Bernard Hoet is an employee of the GSK group of companies and holds shares as part of his employee remuneration. Vidya Arankalle and Monjori Mitra have nothing to disclose.
Figures


References
-
- Global Burden of Disease Study Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet (London, England). 2016;388(10053):1545–1602. doi: 10.1016/S0140-6736(16)31678-6. - DOI - PMC - PubMed
-
- Rakesh PS, Sreelakshmi MK. 84 outbreaks of hepatitis A in last five years in Kerala State—are we resigning to fate? Natl J Res Commun Med. 2017;6(3):267–270.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
