

Technology-assisted rehabilitation following total knee or hip replacement for people with osteoarthritis: a systematic review and meta-analysis
- PMID: 31679511
- PMCID: PMC6825714
- DOI: 10.1186/s12891-019-2900-x
Technology-assisted rehabilitation following total knee or hip replacement for people with osteoarthritis: a systematic review and meta-analysis
Abstract
Background: To evaluate the effectiveness and safety of technology-assisted rehabilitation following total hip/knee replacement (THR/TKR).
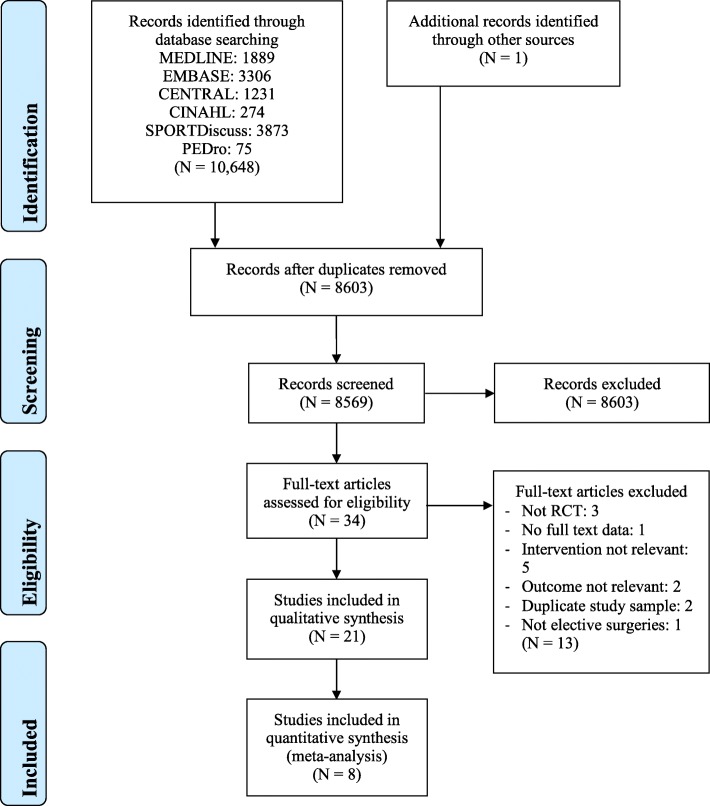
Methods: Six electronic databases were searched without language or time restrictions for relevant studies: MEDLINE, EMBASE, Cochrane Library, CINAHL, SPORTDiscus, Physiotherapy Evidence Database (PEDro); from inception to November 7th, 2018. Two reviewers independently applied inclusion criteria to select eligible randomised controlled trials (RCTs) that investigated the effectiveness of technology-based interventions, compared with usual care or no intervention for people undergoing THR/TKR. Two reviewers independently extracted trial details (e.g. patients' profile, intervention, outcomes, attrition and adverse events). Study methodological quality was assessed using the PEDro scale. Quality of evidence was critically appraised using the Grading of Recommendations, Assessment, Development and Evaluation approach.
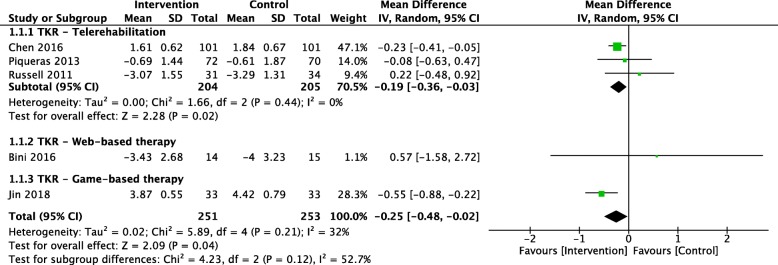
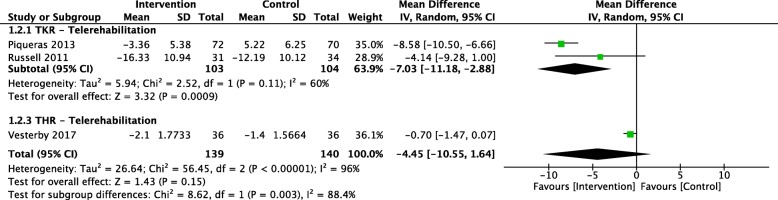
Results: We identified 21 eligible studies assessing telerehabilitation, game- or web-based therapy. There were 17 studies (N = 2188) in post-TKR rehabilitation and 4 studies (N = 783) in post-THR rehabilitation. Compared to usual care, technology-based intervention was more effective in reducing pain (mean difference (MD): - 0.25; 95% confidence interval (CI): - 0.48, - 0.02; moderate evidence) and improving function measured with the timed up-and-go test (MD: -7.03; 95% CI: - 11.18, - 2.88) in people undergoing TKR. No between-group differences were observed in rates of hospital readmissions or treatment-related adverse events (AEs) in those studies.
Conclusion: There is moderate-quality of evidence showed technology-assisted rehabilitation, in particular, telerehabilitation, results in a statistically significant improvement in pain; and low-quality of evidence for the improvement in functional mobility in people undergoing TKR. The effects were however too small to be clinically significant. For THR, there is very limited low-quality evidence shows no significant effects.
Keywords: Digital health; Healthcare delivery; Joint arthroplasty; Telerehabilitation; Virtual reality.
Conflict of interest statement
Professor Hunter provides consulting advice for Pfizer, Lilly, TLC bio and Merck Serono. Associate Professor Manuela L. Ferreira is a member of the editorial board of this journal. All other authors have no competing interests.
Figures

References
-
- Disease GBD, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1545–1602. doi: 10.1016/S0140-6736(16)31678-6. - DOI - PMC - PubMed
-
- Australian Orthopaedic Association National Joint Replacement Registry . Analysis of state and territory health data all arthroplasty, annual report. Adelaide: AOA; 2017.
-
- Royal Australasian College of Surgeons 2018 . Rehabilitation pathways following hip and knee arthroplasty. North Adelaide: Royal Australasian College of Surgeons; 2018.
-
- Christensen C. The innovator's dilemma: when new technologies cause great firms to fail. Boston: Harvard Business Review Press; 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
